

Abstract: Congenital oesophageal duplications are rare anomalies classified under foregut malformations. They represent approximately 20% of all gastrointestinal (GI) duplications, which occur in about 1 in 4,500 live births. Among GI duplications, ileal duplications are the most common, while oesophageal duplications are relatively uncommon, and occur with equal frequency in males and females. The clinical presentation depends on the size and location of the duplication. Many children exhibit non-specific symptoms such as poor weight gain, stunted growth, feeding difficulties, dysphagia, or respiratory issues due to compression of adjacent structures. Early diagnosis through imaging and appropriate surgical management is crucial to prevent complications.
We report the case of a 5-year-old male child weighing 10 kg who presented with stunted growth and progressively worsening dysphagia, more pronounced for solids than liquids, over four years. Imaging findings from thin barium swallow demonstrated a dilated upper oesophagus with stricture at the junction of the upper and mid oesophagus, along with a large hiatal hernia causing upward displacement of the gastro-oesophageal junction and narrowing at this level in the upright position; in the supine position, the paraoesophageal contrast extended up to C5, while the duodenal and proximal bowel loops appeared normal. Contrast-enhanced computed tomography (CT) of the neck, chest, and upper abdomen revealed partial duplication of the proximal and mid oesophagus, with a midline fold or membrane extending approximately 6 cm from C5 to D7, in addition to a dilated lower oesophagus. Cross-functional imaging enabled a non-invasive diagnosis of this rare anomaly and provided crucial anatomical details for planning surgical correction, highlighting the potential for definitive treatment with minimal mediastinal complications.
Key words: Foregut Malformations, Tubular Oesophageal Duplication, Oesophageal Stenosis, Hiatus Hernia.
Introduction
Congenital foregut malformations arise from abnormal embryogenesis of the foregut. Among these, oesophageal duplication is an extremely rare anomaly, accounting for approximately 20% of all alimentary tract duplications, which themselves occur in about 1 in 4,500 live births. Morphologic variants of oesophageal duplications include cystic, tubular and diverticular forms. These anomalies may be associated with other spinal or vertebral malformations and, rarely, congenital diaphragmatic hernia.
This case report describes the imaging evaluation of a tubular oesophageal duplication in a 5-year-old male child presenting with dysphagia and recurrent lower respiratory tract infection (LRTIs). The imaging findings were crucial in pre-operative planning to facilitate surgical management while minimising mediastinal complications.
Case Report
A 5-year-old male child weighing 10 kg presented with failure to thrive and a gradually progressive difficulty in swallowing, more pronounced for solid foods than liquids, for the past four years. This was associated with occasional cough and recurrent LRTIs during the same period. There was no history of prior surgery, corrosive ingestion, or trauma. The child was born at full term via normal vaginal delivery, with an uneventful postnatal course.
On thin barium swallow (Figure 1), there was a dilated upper oesophagus with a stricture at the junction of the upper and mid oesophagus. A hiatus hernia was noted, with upward displacement of the gastrooesophageal junction (GEJ) and narrowing at this level in the standing position. In the supine position, paraoesophageal contrast was seen extending up to the C5 vertebral level, approximately over a length of 7 cm. The remaining bowel loops appeared normal.
On contrast-enhanced computed tomography (CT) of the neck, chest, and upper abdomen (Figures 2 and 3), partial duplication of the proximal and mid oesophagus was seen, with a midline fold or membrane extending approximately 6 cm from the C5 to the D7 vertebral level. The lower oesophagus was dilated. A large hiatal hernia was also identified, along with oesophageal dilatation proximal to the stricture at the junction of the upper and mid oesophagus.

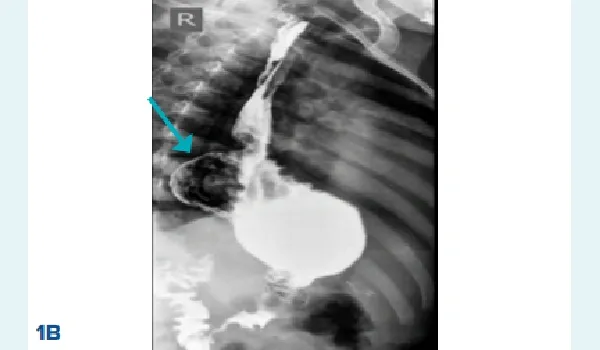
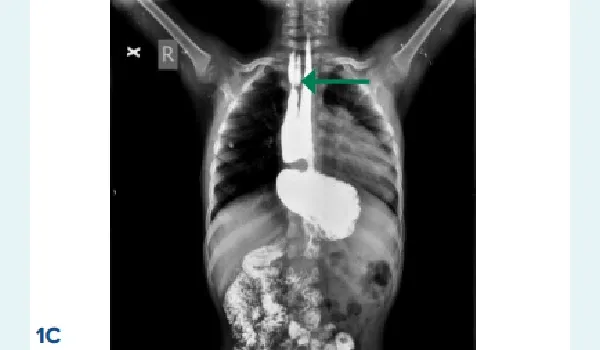
Figure 1: A. Barium anteroposterior (AP) view shows a dilated proximal oesophagus due to stricture (red arrow), B. Barium swallow right anterior oblique (RAO) view shows a large hiatus hernia (blue arrow) with the gastrooesophageal junction (GEJ) located above the diaphragm, C. Barium AP view shows duplicated oesophagus in all 3 radiographs with hiatus hernia and normally visualised small bowel loops (green arrow).
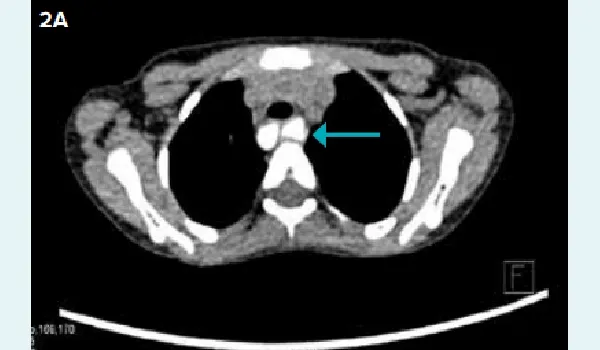

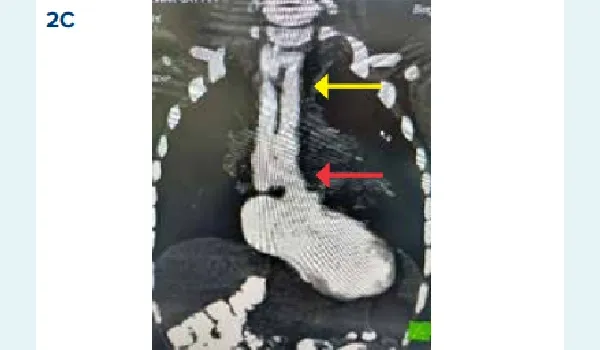
Figure 2A-C: A. Axial section shows dilated oesophageal lumen separated by thick fibrous septa (blue arrow), B. Shows luminal narrowing caused by a stricture (blue arrow), C. Maximum intensity projection (MIP) coronal images show hiatus hernia stricture (red arrow) and oesophageal duplication (yellow arrow).
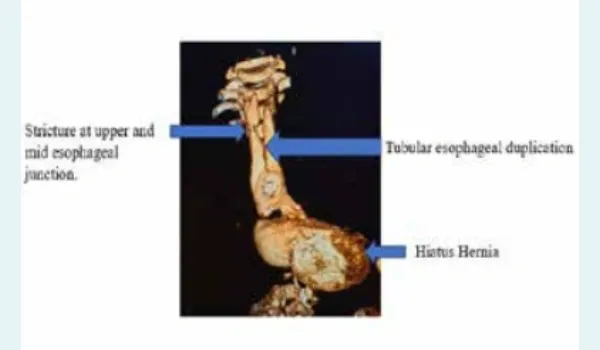
Figure 3: Computed Tomography (CT) neck, chest and upper abdomen with oral contrast using maximum intensity projection (MIP) images confirms the barium swallow findings with no associated vertebral or spinal anomalies.
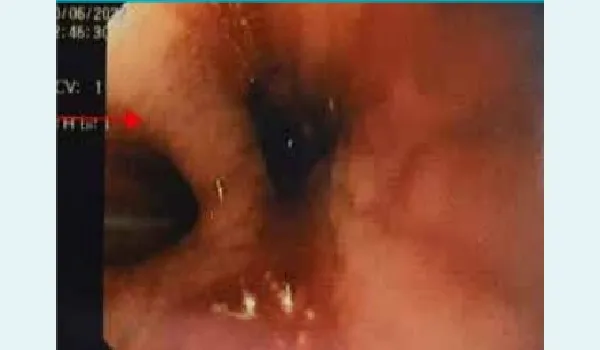
Figure 4: Endoscopy via gastrotomy shows septum/ membrane between the duplicated oesophagus.

Figure 5: Post endoscopic stapler septotomy.

Figure 6: Post-operation virtual reality thoracoscopy (VRT) images reveal resolution of stricture with partial duplication.
Discussion
Congenital foregut malformations are among the rarest developmental anomalies, with gastrointestinal (GI) duplications occurring in approximately 1 in 4,500 live births. Of these, only about 20% involve the oesophagus, making oesophageal duplications particularly uncommon.1,2 They result from aberrations during embryogenesis of the foregut. Although the exact mechanisms of oesophageal duplications are not fully understood, two accepted theories include the diverticular theory and the canalisation defect theory. During the solid stage of foetal intestinal development, around the 6th gestational week, incomplete vacuolisation progressing from the cranial to caudal direction may lead to duplication.3
Oesophageal duplications may be associated with oesophageal atresia, tracheoesophageal fistula (TOF), or vertebral anomalies, such as scoliosis, hemi vertebrae, or spina bifida, in up to 20% of cases. Rarely congenital diaphragmatic hernia may also coexist. The condition occurs equally in males and females. Symptoms usually appear early in life, with most patients presenting before the age of 2 years. Clinical presentation of foregut duplication depends on four main factors:
- The anatomic level or location of the lesion
- Mass effect of the lesion
- Complications secondary to luminal secretions
- Cyst infection
Patients become symptomatic due to respiratory symptoms secondary to airway compression from the mass effect.3,4
There are three morphological types of oesophageal duplication:3,5
- Cystic (most common): May communicate or remain non-communicating with the oesophageal lumen
- Tubular (rare): Communicates with the true oesophageal lumen, often sharing a long segment of its wall, separated by a thick fibrous septum
- Diverticular (rarest): This variant is rarely observed
Oesophageal duplication may occur in the cervical, thoracic or abdominal oesophagus. Tubular duplication can originate in either the thorax or abdomen but are usually located in the lower oesophagus within the posterior mediastinum, projecting into the right or left thorax.1
Histologically, thoracic oesophageal duplication contain purely GI epithelium, even when located remote from the native oesophagus.5
Management depends on the patient’s symptoms. Symptomatic oesophageal duplication cysts are typically excised through thoracoscopy. For partial tubular oesophageal duplications endoscopic stapler septotomy has emerged as a novel, minimally invasive surgical technique (Figures 4, 5 and 6).5 With the advent of newer modalities robotic thoracoscopic excision of oesophageal duplication cysts has also been reported as a valuable option.6
Conclusion:
Tubular oesophageal duplication is a rare congenital anomaly of the foregut. Oesophageal duplications are classified into three types: cystic, tubular and diverticular. Symptoms usually arise when complications develop. A barium swallow is the first-line investigation for a child presenting with dysphagia, while contrastenhanced CT is the investigation of choice for definitive diagnosis.
Abhishekavalli JP, Pran Purohit, Neemish Kamat, Mitusha Verma, Deepak Patkar. Tubular Oesophageal
Duplication: A Difficult Truth to Swallow in a Child with Stunted Growth, Unravelling with Imaging. MMJ.
2025, September. Vol 2 (3).
References
- Trappey AF 3rd, Hirose S. Esophageal duplication and congenital esophageal stenosis. Semin Pediatr Surg. 2017;26(2):78–86.
- Saha AK, Kundu AK. Tubular duplication of the oesophagus presenting with dysphagia. Singapore Med J. 2014;55(6):e90.
- Jacobs IJ, Ku WY, Que J. Genetic and cellular mechanisms regulating anterior foregut and esophageal development. Dev Biol. 2012;369(1):54–64.
- Patiño Mayer J, Bettolli M. Alimentary tract duplications in newborns and children: Diagnostic aspects and the role of laparoscopic treatment. World J Gastroenterol. 2014;20(39):14263–71.
- Kim JH, Kwon CI, Rho JY, et al. Communicating tubular esophageal duplication combined with bronchoesophageal fistula. Clin Endosc. 2016;49(1):81–5.
- Dalvi AV, Save M, Kothari P, et al. Management of tubular oesophageal duplication - A novel approach, J Pediatr Surg Case Rep. 2023;89:102570.