

Abstract:
Myelin oligodendrocyte glycoprotein immunoglobulin G-associated optic neuritis (MOG-IgG ON) typically presents as severe, painful, and recurrent vision loss, often accompanied by optic disc oedema, which can result in significant visual morbidity. We report the case of a 27-year-old female of African ethnicity with a history of headache and bilateral gradual, progressive vision loss. Ophthalmic examination revealed no light perception and stage 3 papilloedema in both eyes. Magnetic resonance imaging (MRI) demonstrated bilateral optic neuritis, and anti-MOG-IgG was positive, confirming a diagnosis of MOG-IgG ON. The patient demonstrated notable visual improvement after the initiation of plasma exchange (PLEX) and high-dose corticosteroids within 53 hours of admission, followed by rituximab therapy. A total of seven sessions of PLEX were conducted, resulting in an improvement of ≥ 2 levels in the visual outcome scores by the end of the seventh session. Ultimately, a visual acuity of 6/6 in each eye was achieved after the administration of two doses of intravenous (IV) rituximab. This case study highlights the critical importance of early PLEX initiation to prevent irreversible optic nerve damage in MOG-IgG ON.
Key words: MOG-IgG–Associated Optic Neuritis, Plasma Exchange, High-Dose Corticosteroid, Rituximab.
Introduction
Optic neuritis (ON), a common cause of acute optic nerve injury in children and adults, is characterised by inflammation of the second cranial nerve.1 It has an annual incidence of 3.9 per 100,000 population.2 A strong female predominance has been observed among individuals who are seropositive for myelin oligodendrocyte glycoprotein immunoglobulin G (MOG-IgG) or anti-aquaporin-4 (AQP4) IgG.3,4 Vision loss due to MOG-IgG ON is typically severe, painful, recurrent, and associated with optic disc oedema.5
The efficacy of plasma exchange (PLEX) is attributed to the removal of circulating autoantibodies and other immunologically active substances (e.g., complement and cytokines) from the blood.6 A trend toward increased usage of PLEX for severe demyelinating attacks, including ON, has been observed.7,8
Early commencement of PLEX is crucial to the clinical outcomes in cases of severe ON.9 Early clinical recognition and initiation of treatment are beneficial for maximum visual recovery. This approach should be directed by early diagnosis of ON and its subtype, prompt administration of high-dose corticosteroids, and the addition of PLEX as second-line therapy. PLEX helps prevent the loss of high-contrast vision, enhances contrast sensitivity, and maintains colour vision and visual fields.1
Improvement in visual function was assessed across ten levels, [Table 1] visual acuity (VA) improvement of ≥ 2 levels was selected as the outcome indicator for visual improvement.
| Level | Clinical Parameter |
|---|---|
| 1 | 20/20 |
| 2 | Scotoma, but better than 20/30 |
| 3 | 20/30 ≥ visual acuity ≥ 20/ 60 |
| 4 | 20/60 ≥ visual acuity ≥ 20/200 |
| 5 | 20/200 ≥ visual acuity ≥ 20/ 800 |
| 6 | 20/800 ≥ visual acuity ≥ 20/2000 |
| 7 | Counting fingers |
| 8 | Hand movement |
| 9 | Light perception |
| 10 | No light perception |
Table 1:Visual outcome score
Case Report
Patient demographics and history: A 27-year-old woman of African ethnicity presented to our institute with complaints of headache localised to the left temporal region. The headache was gradual in onset, holocranial, and persistent throughout the day for the past two weeks. She subsequently developed gradual progressive bilateral vision loss, initially starting with decreased vision in her left eye over one week accompanied with pain on eye movement and blurring of vision, followed by complete loss of vision in both eyes over the subsequent week.
Initial presentation: Ophthalmic examination showed no light perception in either eye. The intraocular pressure was 16 mmHg. The anterior segments of both eyes were within normal limits. Posterior segments showed stage 3 papilloedema bilaterally. Ocular movements were full, and pupils were mid-sized and not reactive.
Investigations: A lumbar puncture was performed, following which transient improvement in vision was observed, which subsequently deteriorated in both eyes. The lumbar puncture and cerebrospinal fluid (CSF) reports were inconclusive.
Ocular coherent tomography (OCT) revealed complete obscuration of all disc margins, obliteration of the cup-to-disc ratio, and increased thickness of the superior and inferior quadrants of the retinal nerve fibre layer (RNFL).
Magnetic resonance imaging (MRI) of the whole brain revealed bilateral hyperintensities in the optic nerves with mild point contrast enhancement, along with mild scleral indentation, suggestive of bilateral optic neuritis with papilloedema (Figure 1).
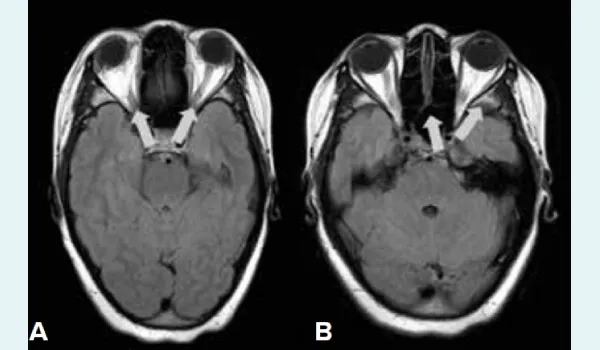
Figure 1. A and B: Magnetic Resonance Imaging (MRI) brain showing hyperintense signal intensity in the bilateral optic nerves with mild post contrast enhancement, along with mild indentation of sclera.
Contrast-enhanced MRI of the whole spine revealed a subtle T2-weighted short tau inversion recovery (T2W/ STIR) hyperintense signal at the cervicomedullary junction and along the anterior aspect of the cervical spinal cord from C2 to C7. No unusual enhancement was observed. Age-commensurate degenerative changes were observed in the rest of the spine (Figure 2).

Figure 2C: Magnetic Resonance Imaging (MRI) spine showing hyperintense signal at the cervicomedullary junction and along the anterior aspect of cervical spinal cord from C2 to C7 vertebral levels.
Serological tests showed anti MOG positivity, and were negative for anti- neuromyelitis optica antibodies (NMO), antineutrophil cytoplasmic antibodies-cytoplasmic and perinuclear (ANCA C and P), and antinuclear antibodies by immunofluorescence (ANA-IF). Visual evoked potential (VEP) revealed prolonged P-100 latency in the right eye and non-recordable P-100 latency in the left.
Management
As per the American Society for Apheresis (ASFA) guideline, PLEX for acute and relapsing attacks is a category II, Grade 1B recommendation, and for maintenance therapy, Category III, Grade 2C, using replacement doses of 1.5 plasma volumes and median of 5 sessions distributed daily or on alternate days over 10 days for acute NO spectrum disorder.10 The Type II category refers to disorders in which apheresis is considered an acceptable second–line therapy, either on its own or combined with other therapies. Meanwhile, Grade 1B indicates a strong recommendation supported by moderate quality evidence.
The patient was started with therapeutic PLEX on alternate days, accompanied by once-daily high dose IV methylprednisolone (IVMP) at 1gm, within 53 hours of admission. A total of seven sessions of PLEX were performed using Spectra Optia® in which 1.5 times the total plasma volume was processed using a combination of albumin, fresh frozen plasma, and normal saline as the replacement fluid. Blood flow was aimed to reach 50-70 ml/kg. Anticoagulant citrate dextrose (ACD) was used as an extracorporeal anticoagulant in the ratio 1:12. Following this, the patient received two doses of 500 mg IV rituximab.
The patient experienced gradual improvement in visual acuity during the PLEX sessions, with improvement of ≥ 2 levels in the visual outcome scores by the end of the seventh session. Eventually, a best-corrected vision of 6/6 in both eyes was achieved after rituximab administration.
Discussion
PLEX is an emerging treatment modality for patients with neurological disorders. It has been effectively used for several decades and has evolved to become more practical, reliable, and associated with reduced complication rates. PLEX in patients with MOG-IgG ON is associated with better outcomes.5,11
PLEX after IVMP is well tolerated. While IVMP remains first line, the combination of IVMP with PLEX can be used in steroid-refractory cases or recurrence of MOG-IgG ON in a previously affected eye, whereas immunosuppressants can be employed to prevent recurrence of MOG-IgG ON.
MOG-IgG seropositivity is associated with a relapsing course of inflammatory ON. Though most patients recover good visual function, predicting future attacks during remission remains an unanswered question.5 Hence, the most effective approach for optimising long-term visual outcome is the prevention of future attacks.8
Conclusion
MOG-IgG ON can lead to severe, painful, and recurrent vision loss. This case highlights the critical importance of early PLEX initiation to prevent irreversible optic nerve damage. The synergistic effect of combining PLEX with corticosteroids and immunotherapy accelerates recovery and preserves visual function, providing a possible treatment solution to achieve restoration of visual acuity.
Priyasha Prajapat, Rasika Dhawan Setia, Mitu Dogra, Rohit Bansil, Amena Ebadur Rahman, Vadad,
Sonia Joseph, Dhriti Ghosh, Garima Katiyar. Therapeutic Plasma Exchange in Myelin Oligodendrocyte
Glycoprotein–Related Optic Neuritis: Restoring Vision Through Early Intervention – A Case Report. MMJ.
2025, June. Vol 2 (2).
References
- Bennett JL. Optic Neuritis. Continuum (Minneap Minn). 2019;25(5):1236-1264.
- Hassan MB, Stern C, Flanagan EP, et al. Population-based incidence of optic neuritis in the era of aquaporin-4 and myelin oligodendrocyte glycoprotein antibodies. Am J Ophthalmol. 2020;220:110-4.
- Jarius S, Paul F, Aktas O, et al. MOG encephalomyelitis: international recommendations on diagnosis and antibody testing. J neuroinflammation. 2018;15(1):134.
- Jurynczyk M, Messina S, Woodhall MR, et al. Clinical presentation and prognosis in MOGantibody disease: a UK study. Brain 2017; 140(12):3128–3138.
- Chen JJ, Flanagan EP, Jitprapaikulsan J, et al. Myelin oligodendrocyte glycoprotein antibody–positive optic neuritis: clinical characteristics, radiologic clues, and outcome. Am J Ophthalmol. 2018;195:8-15.
- Lehmann HC, Hartung HP, Hetzel GR, et al. Plasma exchange in neuroimmunological disorders: Part 1: Rationale and treatment of inflammatory central nervous system disorders. Arch Neurol. 2006;63(7):930-5.
- Bennett JL, Costello F, Chen JJ, et al. Optic neuritis and autoimmune optic neuropathies: advances in diagnosis and treatment. Lancet Neurol. 2023; 22(1):89-100.
- Horton L, Bennett JL. Acute management of optic neuritis: an evolving paradigm. J Neuroophthalmol. 2018;38(3):358-67.
- Fu J, Wang Y, Li H, et al. Efficacy of plasma exchange treatment for demyelinating optic neuritis associated with various serum antibodies: a prospective cohort study. Neurol Ther. 2022;11(2):797-813.
- Connelly-Smith L, Alquist CR, Aqui NA, et al. Guidelines on the use of therapeutic apheresis in clinical practice–evidencebased approach from the Writing Committee of the American Society for Apheresis: the Ninth Special Issue. J Clin Apher. 2023;38(2):77-278.
- Chen JJ, Flanagan EP, Pittock SJ, et al. Visual outcomes following plasma exchange for optic neuritis: an international multicenter retrospective analysis of 395 optic neuritis attacks. Am J Ophthalmol. 2023;252:213-24.