

Abstract:
Complex acetabular fractures, with or without hip dislocation, in elderly or osteoporotic patients present significant surgical challenges. Traditional open reduction and internal fixation (ORIF) frequently fails in this population due to poor bone quality, fracture comminution, and delayed presentation. This case series describes the use of primary total hip arthroplasty (THA) as an alternative treatment strategy in selected cases. The objective was to evaluate the role of arthroplasty-based reconstruction in the management of complex and neglected hip injuries in the elderly population. This case series includes three patients with neglected or complex acetabular fractures, with or without hip dislocation, managed with primary THA. Surgical approaches, implant selection, and reconstruction techniques were individualised for each case. Clinical presentation, surgical strategy, postoperative rehabilitation, and short-term outcomes were analysed. All patients underwent successful arthroplasty-based reconstruction using appropriate techniques, such as acetabular cages and supplementary fixation when indicated. Early mobilisation was achieved in all cases, with ambulation initiated on postoperative day (POD) 1. All patients were discharged on POD 4. Early functional recovery was achieved in all cases with satisfactory radiological alignment and joint congruity. No perioperative complications or revision surgeries were required. Primary THA with appropriate reconstructive techniques offers a reliable and effective alternative to ORIF in complex and neglected hip injuries, particularly in elderly patients. This approach provides immediate joint stability, enables early mobilisation, and reduces morbidity related to failed fixation and prolonged immobilisation.
Key words: Acetabular Fracture, Arthroplasty, Hip Dislocation, Elderly Trauma, Acetabular Cage Reconstruction.
Introduction
The epidemiology of acetabular fractures has shifted towards an ageing population. Current data indicate that approximately 20%–30% of acetabular fractures occur in patients over 60 years of age, and these injuries are increasingly associated with lower-energy trauma such as ground-level falls.1-3 The consequences of delayed or failed fixation in this population are severe. Prolonged immobilisation leads to well-documented complications, including deep vein thrombosis, pulmonary embolism, pressure sores, pneumonia, delirium, and loss of preinjury independence. 4-6
Neglected acetabular fractures and chronic dislocations result in progressive articular cartilage damage, femoral head necrosis, and significant acetabular bone loss. The longer the delay in reduction, the greater the likelihood of irreversible chondral damage, hip instability, and secondary osteoarthritis.4
In selected patients — particularly the elderly, osteoporotic, or those with delayed presentations — total hip arthroplasty (THA) has emerged as a viable and increasingly favoured alternative to open reduction and internal fixation (ORIF). Arthroplasty-based reconstruction offers several distinct advantages: immediate joint stability, pain relief, and, crucially, early mobilisation and weightbearing. In elderly patients, this approach eliminates prolonged bed rest, reducing the risk of venous thromboembolism, pneumonia, and pressure ulcers, while enabling faster functional recovery.7-9
Recent literature supports this paradigm shift. Multiple authors have demonstrated improved early functional outcomes and reduced reoperation rates with acute or delayed THA compared to fixation alone in elderly and low-demand populations with complex acetabular fractures.10,11
The objective of this case series is to demonstrate the application of arthroplasty-based reconstruction in three patients with distinct presentations of complex and neglected hip injuries, highlighting surgical decisionmaking, reconstruction techniques, and early clinical outcomes.
Methods
Patients were selected if they were aged ≥ 70 years and presented with complex acetabular fracture patterns with significant comminution, with or without an associated femoral head fracture and/or osteonecrosis.
Preoperative evaluation included clinical examination, radiographic assessment (plain radiographs and computed tomography [CT]), and comprehensive medical optimisation in consultation with internal medicine and anaesthesia teams. The decision to pursue primary THA rather than ORIF was based on patient age and functional demands, bone quality assessment, fracture complexity, timing of injury, and patient preference following informed discussion of risks and benefits.
All patients underwent THA via a modified lateral approach. After careful capsulotomy and hip dislocation, femoral head viability was assessed, the acetabulum was debrided of pannus and damaged cartilage, and a structural bone graft was harvested from the femoral head or iliac crest as needed. Acetabular cages were used for significant defects, with cemented or uncemented cups selected based on bone quality, and uncemented stems were used in all cases.
All patients were monitored in intensive care postoperatively for one day. Prophylactic anticoagulation was administered as per institutional protocol. Physical therapy commenced on postoperative day (POD) 1, with assisted out-of-bed mobilisation. The weight-bearing protocol consisted of toe-touch weight bearing, advancing to full weight bearing as tolerated. Discharge criteria included adequate pain control, independent transfers, and clear discharge planning.
Primary outcomes assessed included surgical success (completion of planned procedure without major intraoperative complications), early mobilisation (achievement of out-of-bed ambulation by POD 1), length of hospital stay, perioperative complications, and radiological alignment at discharge. No readmissions were recorded up to 180 days post-surgery.
Case Report
Case report 1: Neglected acetabular fracture with central hip dislocation
A 71-year-old male presented to our institution two months after sustaining a mechanical fall at home. At presentation,he reported severe left hip pain, inability to bear weight,and visible limb deformity. Prior treatment at an outside facility had included attempted closed reduction followed by upper tibial pin traction, without improvement in hip position.
On initial evaluation at our centre, the patient reported persistent pain and was completely non-ambulatory (Figure 1A and B).
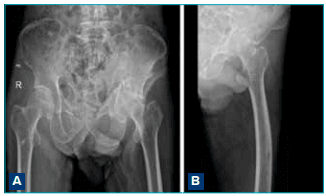
Figure 1A and B: Pelvic radiographs showing a neglected central hip dislocation of the left hip with an associated acetabular fracture pattern consistent with a central acetabular fracture with significant posterior wall involvement. The femoral head remained medially and superiorly displaced, corresponding to Paprosky Type 2C acetabular defect.11
Following comprehensive medical evaluation and clearance, the patient underwent left THA via a modified lateral approach. Key technical points included careful division of the gluteus medius, with anterior and posterior capsular releases to facilitate hip mobilisation (Figure 2) extraction and examination of the femoral head, which confirmed an intact articular surface); extensive removal of pannus and fibrous tissue from the acetabulum; harvest of autogenous bone graft from the resected femoral head for defect reconstruction; acetabular cup placement in near-anatomical position; insertion of a cementless femoral stem; and meticulous soft tissue repair with capsular plication.
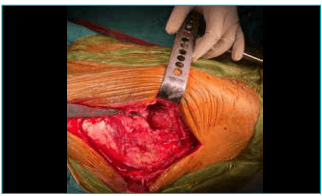
Figure 2: Modified lateral approach — care must be taken while dividing the gluteus medius and during capsulotomy.
The patient tolerated the procedure well, with no intraoperative complications. Postoperative radiographs demonstrated a well-reduced hip with maintained articular congruity and optimal component positioning (Figure 3). The patient was mobilised on POD 1 and progressed rapidly to independent ambulation with a walker. He was discharged on POD 4 with satisfactory pain control and functional mobility. At the final follow-up at four months, radiographs confirmed maintained reduction and appropriate component position.
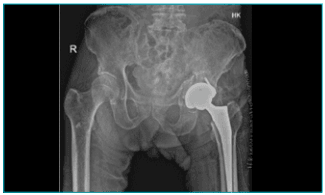
Figure 3: Postoperative X-ray showing reduced acetabular fragment with well-supported acetabular prosthesis and reduced hip joint.
Case report 2: Neglected comminuted acetabular fracture with femoral head involvement
A 73-year-old female presented one month following a fall from standing height. She reported hip pain, inability to bear weight, and progressive functional decline despite attempted conservative management with bed rest and analgesics at a peripheral facility.
Imaging at our institution revealed a chronic, highly comminuted acetabular fracture involving both the anterior and posterior walls, with significant medial wall involvement (Figure 4A and B). A separate fracture line involving the medial femoral head was identified, raising concern for femoral head fracture or impaction injury with consequent femoral head avascularity. The fracture pattern was deemed unsuitable for conventional fixation due to the degree of comminution and femoral head involvement.
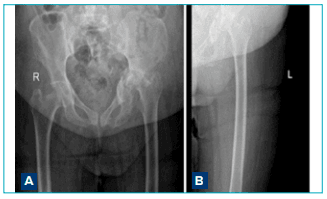
Figure 4A and B Preoperative X-ray showing fracture of the quadrangular plate of the acetabulum with associated anterior and posterior wall fracture. The femoral head is displaced superiorly and medially due to a non-supportive acetabular rim consistent with a Paprosky Type 3B acetabular defect.
The patient, therefore, underwent left THA with acetabular cage reconstruction. The surgical technique was similar in approach, with adequate exposure of the acetabulum. Key steps included identification of the acetabular defect, placement of a structural acetabular cage to span the defect and protect graft incorporation, supplementary bone grafting to support the cage construct, cemented cup placement within the cage, tension band wiring of the greater trochanter to optimise abductor muscle function, and insertion of a cementless femoral stem (Figures 5 and 6). Careful repair of the gluteus medius was performed to maintain the abductor mechanism.

Figure 5:Bone graft harvested from the femoral head.
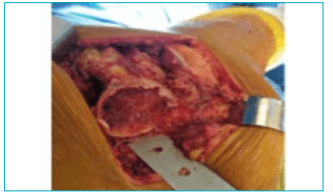
Figure 6: Fragments of the femoral head.
The procedure was completed without major intraoperative complications. Early postoperative radiographs demonstrated appropriate cage positioning, stable cup positioning within the cage, and good bony contact (Figure 7). At follow-up, radiographs showed maintenance of component position, with no evidence of subsidence or loosening.

Figure 7: Postoperative X-ray showing acetabular cage in situ, stabilised with bone graft and screws in situ, along with tensionband wiring of the greater trochanter of the femur.
Case report 3: Neglected anterior column acetabular fracture with protrusio acetabuli in an elderly patient with significant comorbidities
An 83-year-old male with significant medical complexity (diabetes mellitus, hypertension, osteoporosis, early chronic kidney disease, and prior percutaneous transluminal coronary angioplasty) presented following a mechanical fall. He was previously a community ambulator living independently.
Plain radiographs and CT confirmed an anterior column fracture with significant medial wall deficiency and protrusio acetabuli (medial displacement of the acetabulum relative to normal anatomic position)(Figure 8A and B). The acetabular defect was substantial, measuring approximately 2 × 2 cm in the medial wall region. There was no evidence of femoral head fracture.
Given his advanced age, multiple comorbidities, and poor bone quality, primary THA was elected as the most appropriate treatment.
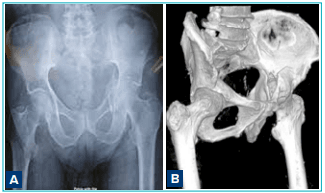
Figure 8A and B:Preoperative imaging revealed an acetabular fracture with severe medial wall involvement and protrusio acetabuli signifying Paprosky type 3B acetabular defect.
The patient underwent left THA with acetabular cage reconstruction and structural bone grafting. Technical nuances included careful preoperative planning to manage protrusio acetabuli and medial wall deficiency; hip dislocation and complete acetabular preparation; harvest of a structural iliac crest bone graft to reconstruct the medial wall defect; careful positioning of the structural graft to restore the hip centre of rotation; placement of a structural acetabular cage to provide load transfer and graft protection; use of morselised bone graft (harvested from the femoral head and iliac crest) to fill residual defects around the cage; cemented cup placement to optimise fixation in osteoporotic bone (Figure 9A–C); insertion of a cementless femoral stem and meticulous soft-tissue repair.
The surgery was completed without any perioperative complications. Postoperative radiographs documented appropriate structural graft incorporation, stable cage positioning, and optimal cup position (Figure 10A and B). The patient was mobilised early and discharged on POD 4. Follow-up radiographs at 12 weeks demonstrated maintained component position and early graft incorporation.
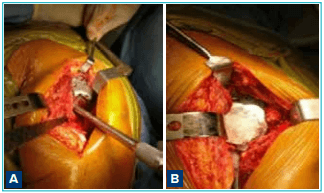
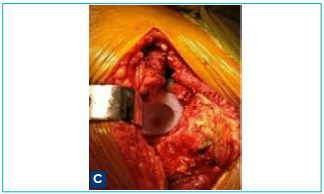
Figure 9A–C:Cage placement along with cemented cup.
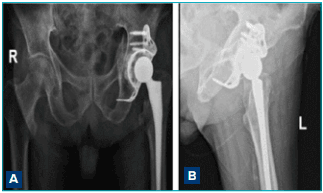
Figure 10A and B:Postoperative radiograph showing stable cage positioning and optimal cup position.
Results
All three patients presented with complex acetabular injuries that had been present for at least one month prior to definitive surgical intervention. All patients were deemed high-risk candidates for conventional ORIF based on advanced age, poor bone quality, fracture complexity,and/or medical comorbidities.
All three patients underwent successful primary THA with appropriate reconstructive techniques. Immediate postoperative radiographs in all three cases demonstrated satisfactory hip reduction, appropriate component positioning (with acetabular and femoral components in neutral to slight anteversion and appropriate offset), maintenance of the hip centre of rotation, and adequate bony contact.
At three months follow-up, radiographs showed maintained reduction, no evidence of component subsidence, and appropriate graft incorporation patterns. Specific surgical techniques are summarised in Table 1. No intraoperative complications, including vascular injury, nerve injury, or significant blood loss requiring transfusion, were observed.
All patients achieved early mobilisation with immediate weight bearing and discharge on POD 4. No perioperative deaths or major complications were documented. At discharge, all patients demonstrated adequate pain control to participate in physical therapy, independent bed-to-chair transfers, and ambulation with a walker or crutches. No patient required readmission within 180 days of discharge
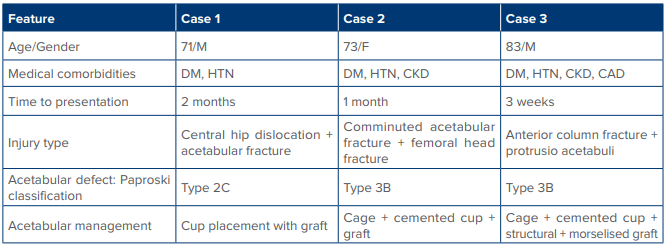
Table 1: Summary of cases and surgical interventions
Abbreviations: CAD: Coronary Artery Disease; CKD: Chronic Kidney Disease; DM: Diabetes Mellitus; F: Female; HTN: Hypertension;M: Male; POD: Postoperative Day.
Discussion
The management of complex and neglected hip injuries remains one of the most challenging problems, particularly in elderly populations. This case series contributes to growing evidence that primary THA, in carefully selected elderly patients with comminuted or neglected acetabular injuries, may offer better functional outcomes compared with late fixation or conversion surgery.Historically, ORIF has been considered the gold standard treatment for acetabular fractures, and this remains true for younger patients with good bone quality and simple fracture patterns. In the elderly osteoporotic cohort with comminuted injuries, however, fixation frequently fails,and late conversion to THA carries higher morbidity.Primary arthroplasty avoids these risks.12 Over the past several decades, the epidemiology of acetabular fractures has shifted towards an older patient population. Ferguson et al. reported that up to 30% of acetabular fractures now occur in patients over 60 years of age, often following low-energy mechanisms such as ground-level falls.2 Elderly patients frequently present with osteoporotic bone, fracture comminution, marginal impaction, and associated medical comorbidities, all of which adversely affect internal fixation stability and healing potential. Anglen et al. described the “gull sign” as a radiographic marker of superior dome impaction and demonstrated its strong association with fixation failure in geriatric acetabular fractures.1 Several authors have since confirmed that osteoporotic bone provides poor screw purchase and reduced load-bearing capacity, leading to secondary displacement, implant failure, and post-traumatic arthritis when ORIF is attempted in this population.1,12 Mears and Velyvis emphasised that delayed reduction significantly increases the risk of irreversible chondral injury, making anatomical reconstruction difficult or impossible.4 In such cases, late ORIF is associated with inferior functional outcomes and a higher likelihood of subsequent conversion to THA. Tannast et al. demonstrated that even in operatively treated acetabular fractures, long-term hip survivorship declines with increasing age, fracture complexity, and delayed intervention.3 These findings underscore the limitations of joint-preserving surgery in elderly or delayed presentations. Koval and Zuckerman highlighted the increased risk of deep vein thrombosis, pulmonary embolism, pneumonia, pressure ulcers, delirium, and loss of independence associated with prolonged immobilisation following hip injuries in older adults.5 These complications contribute to increased morbidity, mortality, and healthcare utilisation. Rickman et al., in a systematic review, reported that fixation combined with or replaced by primary arthroplasty resulted in improved early mobilisation, reduced reoperation rates, and acceptable complication profiles in elderly patients.6 Similarly, Carroll et al. found that patients treated with arthroplasty achieved faster functional recovery and shorter hospital stays compared to those managed with fixation alone.7 Herscovici et al. described the “combined hip procedure,” which integrates limited fixation with immediate THA, allowing restoration of stability while enabling early weight bearing.8 This approach has gained acceptance for complex fracture patterns involving both columns, femoral head injury, or marginal impaction. The use of cages and bone grafting has been shown to be particularly effective in elderly patients with medial wall defects or severe comminution, where conventional press-fit fixation is unreliable. Laflamme et al. highlighted the technical challenges of fixing osteoporotic acetabular fractures involving the quadrilateral plate and emphasised the limitations of fixation alone in such scenarios.9 Arthroplasty in the setting of acetabular fractures often necessitates advanced reconstructive techniques due to bone loss, medial wall deficiency, or protrusio acetabuli. Paprosky et al. provided a widely accepted classification of acetabular defects and outlined reconstructive strategies including the use of acetabular cages, reinforcement rings, and structural bone grafting.11 These constructs allow load transfer to intact pelvic bone, protect graft incorporation, and provide immediate implant stability. An important advantage of primary THA is the avoidance of secondary conversion surgery following failed fixation. Morison et al. demonstrated that THA performed after failed acetabular fracture fixation is associated with higher complication rates, lower implant survivorship, greater blood loss, and greater technical difficulty than primary arthroplasty.13 These findings support the hypothesis that, in selected patients, early arthroplasty may be a more definitive and safer option. This case series presents short-term outcomes only. Longterm implant survival, the trajectory of any underlying osteoarthritis, and the durability of reconstruction require extended follow-up, which was not available for comprehensive assessment in all patients. Additionally, the series is small (n = 3) and is subject to selection bias toward more complex cases. Prospective comparative studies would further strengthen the evidence base in this domain.
Acknowledgement
We would like to express our sincere gratitude to the Department of Orthopaedics, along with the associated anaesthesiology, physiotherapy and nursing teams for their invaluable support in the perioperative management and the rehabilitation of the patients included in this case. We also acknowledge the contribution of the Department of Radiology for their assistance with imaging and documentation.
We extend our appreciation to the patients and their families for their cooperation and consent, which made this study possible. We are also grateful to the institutional support staff for facilitating clinical data collection and postoperative follow-up.
Funding
No external funding was received for this study.
Conclusion:
This case series demonstrates that primary THA with appropriate reconstructive techniques is a reliable, effective, and increasingly preferred treatment strategy for complex and neglected hip injuries, particularly in elderly, osteoporotic, or low-demand patients. Arthroplasty provides immediate joint stability, facilitates early mobilisation, reduces perioperative morbidity, and prevents the adverse outcomes associated with fixation failure. Based on these findings, a paradigm shift toward greater use of primary THA in carefully selected elderly patients with complex, neglected, or osteoporotic acetabular injuries is supported. Primary THA in this population reduces complications, improves early functional outcomes, and avoids the morbidity associated with fixation failure.
Sana Parveen, Chandeep Singh, Shitij Kacker, Sanjiv Kumar Singh Marya. Surgical Management of Complex and Neglected Hip Injuries Using Arthroplasty-Based Reconstruction. MMJ. 2026, March. Vol 3 (1).
March. Vol 3 (1).
References
- Anglen JO, Burd TA, Hendricks KJ, et al. The "Gull Sign": A harbinger of failure for internal fixation of geriatric acetabular fractures. J Orthop Trauma. 2003;17(9):625–34.
- Ferguson TA, Patel R, Bhandari M, et al. Fractures of the acetabulum in patients aged 60 years and older: An epidemiological and radiological study. J Bone Joint Surg Br. 2010;92(2):250–7
- Tannast M, Najibi S, Matta JM. Two to twenty-year survivorship of the hip in 810 patients with operatively treated acetabular fractures. J Bone Joint Surg Am. 2012;94(17):1559–67.
- Mears DC, Velyvis JH. Acute total hip arthroplasty for selected displaced acetabular fractures: Two to twelve-year results. J Bone Joint Surg Am. 2002;84(1):1–9.
- Koval KJ, Zuckerman JD. Hip fractures: I. Overview and evaluation and treatment of femoral-neck fractures. J Am Acad Orthop Surg. 1994;2(3):141–9
- Rickman M, Young J, Trompeter A, et al. Managing acetabular fractures in the elderly with fixation and primary arthroplasty: A systematic review. Bone Joint J. 2014;96- B(3):291–8.
- Carroll EA, Huber FG, Goldman AT, et al. Treatment of acetabular fractures in an older population. J Orthop Trauma. 2010;24(10):637–44.
- Herscovici D Jr, Lindvall E, Bolhofner B, et al. The combined hip procedure: Open reduction internal fixation combined with total hip arthroplasty for the management of acetabular fractures in the elderly. J Orthop Trauma. 2010;24(5):291–6.
- Laflamme GY, Hebert-Davies J, Rouleau D, et al. Internal fixation of osteoporotic acetabular fractures involving the quadrilateral plate. J Orthop Trauma. 2011;25(2):76–82.
- Giannoudis PV, Grotz MRW, Papakostidis C, et al. Operative treatment of displaced fractures of the acetabulum: A metaanalysis. J Bone Joint Surg Br. 2005;87(1):2–9
- Paprosky WG, Perona PG, Lawrence JM. Acetabular defect classification and surgical reconstruction in revision arthroplasty. Clin Orthop Relat Res. 1994;(298):66–81.
- Mears DC. Management of acetabular fractures in the elderly. J Bone Joint Surg Am. 1999;81(6):819–31.
- Morison Z, Moojen DJ, Nauth A, et al. Total hip arthroplasty after acetabular fracture is associated with lower survivorship and more complications. Clin Orthop Relat Res. 2016;474(2):392–8.