

Abstract:
Steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT) is a rare but potentially reversible autoimmune neurological disorder characterised by a wide spectrum of neuropsychiatric manifestations, seizures, and encephalopathy. Owing to its protean clinical presentation and frequently nonspecific conventional investigations, SREAT is often misdiagnosed as a primary psychiatric illness or cryptogenic epilepsy. We report a case of a young male presenting with acute psychosis in whom multimodal neuroimaging using contrastenhanced magnetic resonance imaging (MRI) of the brain and 18F-fluorodeoxyglucose-positron emission tomography (FDG-PET)/computed tomography (CT) revealed limbic and functional cerebral involvement, respectively. Early recognition and prompt immunotherapy resulted in significant clinical improvement. This case highlights the complementary role of structural and functional neuroimaging in establishing the diagnosis of SREAT. The patient was initially misdiagnosed as schizophrenia due to predominant hallucinations and cognitive decline in the absence of overt seizures, highlighting the diagnostic challenge posed by autoimmune encephalopathies with psychiatric presentations.
Key words: Steroid-Responsive Encephalopathy, Autoimmune Thyroiditis, Hashimoto Encephalopathy, FDG-PET/CT, Limbic Encephalitis, Psychosis, Seizures.
Introduction
Steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT), also referred to as Hashimoto’s encephalopathy, is an uncommon immunemediated encephalopathy associated with elevated thyroid autoantibodies, independent of thyroid hormone status.1,2 Since its initial description, SREAT has remained a diagnostic challenge due to its heterogeneous clinical manifestations and lack of disease-specific biomarkers. Patients may present with cognitive decline, altered behaviour, psychosis, seizures, movement disorders, stroke-like episodes, or fluctuating consciousness.1-3
The diagnosis of SREAT is largely one of exclusion. Cerebrospinal fluid (CSF) analysis is often normal or shows mild protein elevation, while magnetic resonance imaging (MRI) findings range from normal to subtle, nonspecific abnormalities. Electroencephalography (EEG) commonly demonstrates diffuse slowing with or without epileptiform discharges, reflecting underlying encephalopathy. In recent years, functional neuroimaging using 18F-fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT) has gained importance in demonstrating cerebral metabolic dysfunction in autoimmune encephalopathies, particularly when structural imaging is inconclusive.3,4
We describe a case of SREAT in a young male presenting with acute psychosis and refractory seizures, where combined MRI brain and FDG-PET/CT findings played a pivotal role in diagnosis and management.
Case Report
A 24-year-old male with no prior history of psychiatric illness, epilepsy, or systemic disease presented with acute psychosis. The patient had initially been evaluated by a psychiatrist and was diagnosed with schizophrenia based on prominent neuropsychiatric manifestations, including persistent visual and auditory hallucinations, behavioural disorganisation, and progressive cognitive decline. He had been receiving antipsychotic treatment for several months with minimal clinical improvement. Notably, there was no history of overt seizures, convulsive episodes, or loss of consciousness, which initially reduced suspicion for an underlying epileptic or organic encephalopathic process.
However, the subacute onset of fluctuating confusion, worsening cognitive impairment, and prominent hallucinations in a young male, along with poor response to standard antipsychotic therapy, raised concern for a possible organic and autoimmune aetiology rather than a primary psychotic disorder. The absence of classical seizure activity did not exclude the diagnosis, as autoimmune encephalopathies, particularly SREAT, are well known to present predominantly with psychiatric symptoms, altered mental status, and cognitive decline,sometimes in the absence of seizures.
This diagnostic reconsideration prompted further neurological evaluation, including neuroimaging, EEG, metabolic work-up, and autoimmune testing, ultimately leading to the diagnosis of SREAT and subsequent dramatic response to corticosteroid therapy.
On examination, the patient was conscious but confused, with markedly altered behaviour. He responded intermittently to verbal commands and exhibited no focal motor deficits. Vital parameters were stable. Routine laboratory investigations, including metabolic and infectious work-up, were normal.
EEG revealed diffuse background slowing with intermittent epileptiform discharges, suggestive of an underlying encephalopathic process with cortical irritability. CSF analysis showed normal cell counts and biochemistry, effectively excluding infectious encephalitis.
Autoimmune evaluation revealed markedly elevated antithyroglobulin antibody titres, while anti-thyroid peroxidase antibodies and thyroid function tests were within normal limits.
In view of the clinical presentation and EEG findings, autoimmune encephalopathy was suspected, and neuroimaging was pursued.
Neuroimaging findings
MRI of the brain demonstrated subtle bilateral hippocampal and mesial temporal T2-fluid-attenuated inversion recovery (FLAIR) hyperintensities with mild patchy post-contrast enhancement (Figure 1). There was no associated mass effect, diffusion restriction, or haemorrhage. These findings were suggestive of limbic involvement, a pattern commonly seen in autoimmune encephalopathies. The subtlety of MRI abnormalities underscored the limitations of relying solely on structural imaging in such cases.
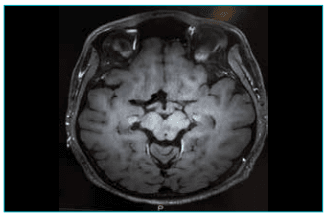
Figure 1: Magnetic resonance imaging (MRI) of the brain (contrast-enhanced): Subtle T2-fluid-attenuated inversion recovery (FLAIR) hyperintensities seen in bilateral hippocampi with patchy contrast enhancement.
Whole-body FDG-PET/CT was performed to evaluate cerebral metabolism and to exclude occult malignancy. PET imaging revealed diffuse hypometabolism of the cerebral cortex, with relative preservation and hypermetabolism of the bilateral basal ganglia and occipital cortex (Figure 2). Fused PET-CT images demonstrated no corresponding structural abnormality on CT. No hypermetabolic lesion suggestive of malignancy was identified elsewhere in the body.
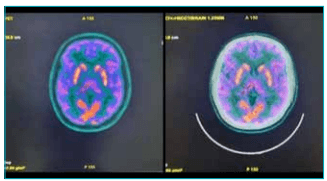
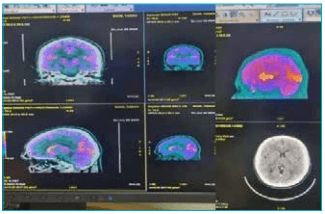
Figure 2: Whole-body 18F-fluorodeoxyglucose-positron emission tomography (FDG-PET)/computed tomography (CT) scan: Diffuse relatively increased/preserved FDG uptake in bilateral basal ganglia and occipital lobe (visual cortex), relative to suppressed FDG uptake in the rest of the cerebral cortex. No other significant focal hypermetabolic lesions in the FDG-PET/CT of the brain were identified.
This metabolic pattern strongly supported an immunemediated encephalopathy and effectively excluded paraneoplastic encephalitis. The occipital cortical involvement correlated with the patient’s visual hallucinations, while basal ganglia hypermetabolism explained the prominent behavioural disturbance and seizure propensity.
Management and outcome
Based on the clinical features, EEG abnormalities, elevated thyroid autoantibodies, limbic MRI changes, and characteristic FDG-PET/CT findings, a diagnosis of SREAT was established.
The patient was initiated on intravenous methylprednisolone (1 g/day for 5 days). Although partial improvement was observed, given the severity of symptoms and PET evidence of widespread functional involvement, intravenous immunoglobulin (IVIG) was administered. Following immunotherapy, the patient showed marked and sustained clinical improvement, with resolution of hallucinations, normalisation of behaviour, and improved seizure control. He was discharged on tapering oral steroids and maintenance antiepileptic medications.
Discussion
SREAT is a rare but important differential diagnosis in patients presenting with acute psychosis and refractory seizures, particularly when routine investigations are unrevealing.1,2 Misdiagnosis as schizophrenia or functional psychiatric illness is common, leading to delays in appropriate therapy and prolonged morbidity.2
Thyroid autoantibodies in SREAT are considered markers of immune dysregulation rather than direct pathogenic agents, and antibody titres do not correlate with disease severity.2,5 Normal thyroid function tests, as seen in our patient, do not exclude the diagnosis.1,5
MRI findings in SREAT are often subtle or nonspecific, as demonstrated in this case.2 EEG abnormalities, though nonspecific, provide an important clue to the encephalopathic nature of the illness.1 FDG-PET/CT plays a crucial complementary role by demonstrating functional cerebral abnormalities that may precede or exceed structural changes.4 The pattern of diffuse cortical hypometabolism with basal ganglia and occipital hypermetabolism has been described in autoimmune encephalopathies and correlates well with neuropsychiatric manifestations.3,4
Importantly, whole-body PET/CT also aids in excluding paraneoplastic aetiologies, thereby guiding appropriate immunotherapy.3
Conclusion:
This case highlights SREAT as a reversible cause of acute psychosis and refractory seizures in young adults. A high index of suspicion, combined with multimodal neuroimaging using MRI of the brain and FDG-PET/CT, is essential for early diagnosis. Prompt immunotherapy can result in dramatic clinical recovery and prevent long-term neurological and psychiatric sequelae.1,3
Anand Kumar Saxena. Steroid-Responsive Encephalopathy Associated with Autoimmune Thyroiditis:
Case Report – Significance of History, Suspicion, and Imaging. MMJ. 2026, March. Vol 3 (1).
References
- Castillo P, Woodruff B, Caselli R, et al. Steroid-responsive encephalopathy associated with autoimmune thyroiditis. Arch Neurol. 2006;63(2):197–202.
- Chong JY, Rowland LP, Utiger RD. Hashimoto encephalopathy: syndrome or myth? Arch Neurol. 2003;60(2):164–71.
- Graus F, Titulaer MJ, Balu R, et al. A clinical approach to diagnosis of autoimmune encephalitis. Lancet Neurol. 2016;15(4):391–404.
- Ferracci F, Carnevale A. The neurological disorder associated with thyroid autoimmunity. J Neurol. 2006;253(8):975–984.
- Moreno-Ajona D, Prieto E, Grisanti F, et al. 18F-FDG-PET Imaging Patterns in Autoimmune Encephalitis: Impact of Image Analysis on the Results. Diagnostics (Basel). 2020;10(6):356.