

Abstract:
Clinical medicine has undergone a paradigm shift over the past few decades, with diagnostic imaging and laboratory investigations increasingly dominating clinical decision-making. While these advances have undoubtedly improved diagnostic precision, they have also contributed to a gradual erosion of bedside examination skills. Many classical clinical signs — once central to diagnosis — are now rarely sought or taught in routine practice. This review revisits the relevance of physical signs in modern medicine, explores why they have been neglected, and highlights nine important but underutilised clinical signs across multiple systems. Each sign is discussed with respect to its historical origins, method of elicitation, pathophysiological basis, and current clinical relevance. Two newly described signs—the ‘Pruritic polished nail sign’ and the ‘Hepatic scratch transmission sign’ — are also introduced as original contributions to contemporary clinical semiology.
Key words: Clinical Signs, Bedside Medicine, Physical Diagnosis, Forgotten Signs, Medical Education.
Introduction
The foundation of clinical medicine lies in careful observation. For centuries, physicians relied almost exclusively on history-taking and physical examination to arrive at a diagnosis. The great clinicians of the past — Hippocrates, Sydenham, Laennec, and Osler — emphasised that “the patient is the textbook,” and that disease reveals itself through patterns of symptoms and signs.1,2
The invention of the stethoscope by René Laennec in 1816 marked the beginning of systematic physical diagnosis. Over the next century, numerous clinical signs were described, each representing an attempt to correlate external physical findings with internal pathology. These signs formed the backbone of bedside medicine well into the mid-20th century.1,2
However, the last five decades have witnessed a dramatic transformation. Modern clinicians now have immediate access to ultrasound, computed tomography (CT), magnetic resonance imaging (MRI), echocardiography, endoscopy, and molecular diagnostics. While these tools have revolutionised care, they have also subtly displaced bedside skills from the centre of clinical practice.1,2
Why Have Clinical Signs Been Forgotten?
Several factors have contributed to the decline of physical diagnosis:1,2
Technological dependence
The availability of imaging and laboratory tests has reduced reliance on clinical reasoning. Diagnosis is often investigation-first rather than examination-first.
Time constraints
High patient volumes and administrative burdens leave little time for detailed bedside examination.
Educational shifts
Medical training increasingly prioritises protocols, algorithms, and test interpretation over physical signs.
Perceived inferiority
Some signs lack high sensitivity or specificity and are therefore considered inferior to imaging.
Defensive medicine
Clinicians rely on investigations for medicolegal documentation rather than clinical judgment.
Why Clinical Signs Still Matter
Despite these challenges, clinical signs remain indispensable:1,2
- They provide immediate diagnostic clues
- They are cost-free and universally available
- They enhance clinical reasoning and pattern recognition
- They reduce unnecessary investigations
- They strengthen the doctor–patient relationship
- They are critical in resource-limited settings
Clinical signs should not compete with technology; rather, they should guide the intelligent use of technology.
Nine Important but Underappreciated Clinical Signs
1. Hutchinson’s sign (Dermatology/Neurology)
First described: Sir Jonathan Hutchinson, 1864.
Description: Vesicular lesions on the tip of the nose in herpes zoster.
Pathophysiology: Involvement of the nasociliary branch of the ophthalmic division of the trigeminal nerve.
Clinical significance: Strong predictor of herpes zoster ophthalmicus and corneal involvement. 3
Modern relevance: A simple inspection sign that determines the urgency of ophthalmology referral (Figure 1).
2. Coin test for pneumothorax (Respiratory medicine)
First described: Late 19th-century European clinical practice, pre-radiography era.
Method: Two coins are tapped on one side of the chest while auscultating the opposite side.
Positive sign: Metallic “ringing” resonance.
Pathophysiology: Air in the pleural space conducts sound efficiently.3
Clinical significance:Suggests pneumothorax, especially in trauma settings (Figure 2).1,2

Figure 1: Hutchinson’s sign.
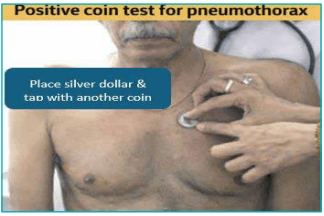
Figure 2: Coin test for pneumothorax.
3. Cruveilhier–Baumgarten sign (Gastroenterology)
First described: Jean Cruveilhier (1835); elaborated by Paul Baumgarten (1907).
Description: Venous hum heard over the epigastrium or umbilicus.
Pathophysiology: Recanalisation of the umbilical vein in portal hypertension.
Clinical significance:Indicates portal hypertension with portosystemic shunting (Figure 3).4
4. Renal bruit (Nephrology)
First correlated with disease: Goldblatt experiments,1934.
Description: Systolic bruit over flanks or epigastrium.
Pathophysiology: Turbulent flow in renal artery stenosis.
Clinical significance:Suggests renovascular hypertension (Figure 4).5

Figure 3: Cruveilhier–Baumgarten Sign.
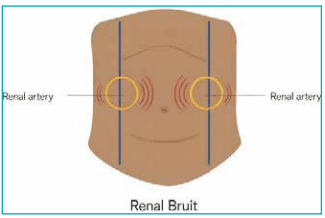
Figure 4: Auscultation over the flank and epigastrium to detect renal bruit suggestive of renal artery stenosis.
5. Plummer’s nails (Endocrinology)
First described: Henry Stanley Plummer, 1912.
Description: Onycholysis — distal separation of nail from nail bed.
Seen in: Graves’ disease, psoriasis, trauma.
Clinical significance: Subtle but classic sign of thyrotoxicosis (Figure 5).6
6. Ewart’s sign (Cardiology)
First described: William Ewart, 1896.
Description: Dullness and bronchial breathing in the left infrascapular region.
Pathophysiology: Compression of the lung by a large pericardial effusion.
Clinical significance: Suggests massive pericardial effusion (Figure 6).7

Figure 5: Plummer’s Nails.
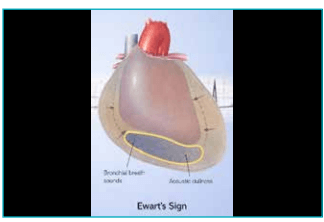
Figure 6: Ewart’s sign.
7. Auscultatory signs of aortic regurgitation (Cardiology)
First systematically described: Austin Flint, mid-19th century.
Key auscultatory signs include:
- Early diastolic decrescendo murmur (best heard at left sternal border).
- Austin Flint murmur: Mid-diastolic rumble at the apex due to regurgitant jet hitting the anterior mitral leaflet.
- Duroziez sign: To-and-fro murmur over the femoral artery.
- Traube’s sign: Pistol-shot sounds over the femoral artery.
Pathophysiology: High stroke volume with rapid diastolic runoff.
Clinical significance: Together, these signs indicate severe aortic regurgitation.8
8. Caput medusae (Gastroenterology)
First described: Ancient Greek medicine; formalised in the 18th century
Description: Dilated periumbilical veins radiating outwards.
Pathophysiology: Portal hypertension with collateral flow.
Clinical significance: Suggests advanced chronic liver disease (Figure 7).

Figure 7: Caput medusae.
9. Plantar reflex variants (Neurology)
First systematically described: Joseph Babinski, 1896.
Variants include:
- Babinski: Upgoing great toe
- Chaddock (1911): Stroking the lateral malleolus
- Oppenheim (1902): Stroking tibial crest
- Gordon (1904): Squeezing the calf muscle
- Schaefer: Achilles compression
Clinical significance: Upper motor neuron lesion.
Modern relevance: Still the most reliable bedside sign of corticospinal tract dysfunction.8
Pathophysiology: High stroke volume with rapid diastolic runoff.
Clinical significance: Together, these signs indicate severe aortic regurgitation.8
Novel Clinical Signs Described by Prof.Narinderpal Singh
1. Shiny nail sign (Pruritus nail sign) in obstructive jaundice
Definition: In patients with chronic cholestasis and obstructive jaundice, persistent generalised pruritus leads to repeated rubbing and scratching of the nails against clothing, skin, or bed linen. Over time, this results in abnormally smooth, glossy, and polished nails.
Clinical significance: The presence of unnaturally shiny nails in a jaundiced patient is an indirect marker of severe, long-standing cholestatic pruritus and suggests obstructive pathology rather than hepatocellular jaundice (Figure 8).
Proposed name: Pruritic polished nail sign (or cholestatic shiny nail sign) This sign was originally described by the author based on over 35 years of clinical experience in internal medicine.

Figure 8: Shiny nail sign.
2. Scratch auscultation sign for liver span
Definition: This is a bedside method to estimate liver size by sound transmission.
Method: Place the diaphragm of the stethoscope over the right upper quadrant, just below the costal margin (over the presumed liver area).
- Using a fingernail, gently scratch the abdominal wall starting from the right lower abdomen and move upward towards the costal margin.
- A sudden change in sound intensity and clarity is heard when the scratching reaches the surface of the liver, because sound is transmitted better through solid organ tissue than through bowel and air.
Clinical significance: This helps identify the inferior border of the liver when percussion is difficult (obesity, tense abdomen, ascites).
Proposed name: Hepatic scratch transmission sign (commonly referred to as scratch test for liver span).This bedside sign was conceptualised and refined by the author through extensive clinical observation over more than three decades of medical practice.
Discussion
These signs span neurology, cardiology, hepatology, nephrology, endocrinology, and respiratory medicine. None of these signs replace investigations, but all precede them intelligently. They transform clinicians from test interpreters into clinical thinkers.
Physical diagnosis trains:
- Pattern recognition
- Hypothesis formation
- Anatomical reasoning
- Bedside empathy
Conclusion:
Clinical signs represent the intellectual heritage of medicine. They are not relics but living tools that connect modern clinicians to centuries of observational wisdom. Technology should confirm, not replace, the bedside examination. Reviving clinical signs restores balance between science and art, ensuring that medicine remains a human discipline rather than a purely technological one.
Narinderpal Singh. Clinical Signs – The Forgotten Art! A Review for Postgraduate Medical Students.
MMJ. 2026, March. Vol 3 (1).
References
- Bickley. Bates' Guide to physical examination and history taking. 12th Edition. Philadelphia: Lippincott; 2017.
- Talley NJ, O’Connor S. Clinical examination: a systematic guide to physical diagnosis. 7th Edition. Sydney: Elsevier; 2014.
- Minor M, Gurnani B, Payne E. Herpes Zoster Ophthalmicus. [Updated 2025 Sep 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available at: https:// www.ncbi.nlm.nih.gov/books/NBK557779/. Accessed on: 25th January 2026.
- Masoodi I, Farooq O, Singh R, et al. Courveilhier baumgarten syndrome: a rare syndrome revisited. Int J Health Sci (Qassim). 2009;3(1):97–9.
- Goldblatt H, Lynch J, Hanzal RF, et al. STUDIES ON EXPERIMENTAL HYPERTENSION : I. THE PRODUCTION OF PERSISTENT ELEVATION OF SYSTOLIC BLOOD PRESSURE BY MEANS OF RENAL ISCHEMIA. J Exp Med. 1934;59(3):347–79.
- Toro-Tobon D, Stan MN. Graves’ Disease and the Manifestations of Thyrotoxicosis. [Updated 2024 Sep 24]. In: Feingold KR, Adler RA, Ahmed SF, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available at: https:// www.ncbi.nlm.nih.gov/books/NBK285567/. Accessed on: 25th January 2026.
- Willner DA, Goyal A, Grigorova Y, et al. Pericardial Effusion. [Updated 2024 Jul 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https:// www.ncbi.nlm.nih.gov/books/NBK431089/. Accessed on: 25th January 2026.
- Walker HK. The Plantar Reflex. In: Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd Edition. Boston: Butterworths; 1990. Chapter 73. Available at: https://www.ncbi.nlm.nih.gov/ books/NBK397/. Accessed on: 25th January 2026.