

Abstract:
Plaque brachytherapy is a well-established, eye-preserving treatment for selected intraocular tumours. It delivers a high radiation dose directly to the tumour with rapid dose fall-off, thereby minimising exposure to adjacent critical ocular structures. We report the successful introduction of ruthenium-106 (¹⁰⁶Ru) plaque brachytherapy at Max Super Speciality Hospital, Saket, New Delhi and describe our initial experience.
A 41-year-old male diagnosed with choroidal melanoma on clinico-radiological evaluation was planned for ocular brachytherapy. The procedure was performed under general anaesthesia with strict radiation safety protocols and multidisciplinary coordination. Radiation dose and other parameters were decided based on clinico-radiological parameters. Plaque insertion and removal were uneventful.
Published literature supports high local control rates and acceptable toxicity profiles with ¹⁰⁶Ru plaque therapy, despite high scleral surface doses. Our experience demonstrates that plaque brachytherapy is a feasible, effective, and vision-sparing modality. Establishing such a programme requires institutional commitment, trained personnel, and close collaboration among ophthalmology, radiation oncology, medical physics, and radiation safety teams.
Key words: Plaque Brachytherapy, Ruthenium-106, Uveal Melanoma, Choroidal Melanoma, Ocular Oncology.
Introduction
Plaque brachytherapy is a specialised form of brachytherapy used for treating certain intraocular tumours. It refers to the process of using a low-energy radioactive source (plaque) as a temporary interstitial implant and suturing it to the scleral surface of the eye overlying the tumour. This allows for high doses of radiation to be delivered directly to the tumour, with rapid dose fall-off to surrounding normal tissues, resulting in minimal radiation-induced damage to nearby sensitive normal structures.1
Indications
Its role in uveal melanoma is evolving as it serves as an alternative to enucleation. It is especially indicated for medium-sized tumours (e.g., 2.5–10 mm height). Other indications include retinoblastoma, conjunctival melanomas, iris melanomas, choroidal haemangiomas, and ocular surface tumours like conjunctival squamous cell carcinoma. Plaque brachytherapy is of interest in these tumours as it is an effective, globe-sparing, and consequently vision-preserving treatment that provides good tumour control and a high rate of survival.2
Radioisotopes used for plaque treatment3
- Iodine-125 (125I) – Emits low-energy gamma rays;widely used due to predictable dosimetry and suitable penetration for medium and thicker tumours.
- Ruthenium-106 (106Ru) – A beta emitter with a steep dose fall-off, particularly useful for thinner lesions.
- Palladium-103 (103Pd) – A photon emitter with a short half-life that may reduce radiation exposure to non-target tissues.3
Each radionuclide has distinct dosimetric properties that influence dose distribution, penetration depth, and duration of treatment. The choice of radionuclide depends on tumour size, thickness, and proximity to critical structures such as the macula and optic nerve.4 Plaque brachytherapy requires a multidisciplinary team consisting of radiation oncologists, ophthalmologists, medical physicists, and radiation safety officers for the successful application and implementation of treatment (Figure 1). Treatment planning is guided by detailed imaging (ultrasound, fundus photography) to define various tumour characteristics like tumour dimensions, location, and depth.

Figure 1: The “Ocular Brachytherapy Team” at Max Super Speciality Hospital, Saket, New Delhi.
Case Report
A 41-year-old gentleman presented to the ophthalmology outpatient department (OPD) with complaints of decreased vision in the right eye. He was evaluated for his complaints and underwent further testing. On detailed clinical examination, his right-sided visual acuity was 6/12. Fundoscopy revealed a large mass in the superotemporal quadrant with exudative retinal detachment. Based on the clinico-radiological assessment, the diagnosis of right choroidal melanoma was established. Further treatment options, including plaque brachytherapy, particle beam therapy, and enucleation, were discussed in detail. The patient was keen on preserving vision, and he was planned for right eye plaque brachytherapy procedure with a 106Ru source. The tumour specifications were assessed with ultrasound, and the tumour thickness was found to be 13.5 mm with an apical height of 9.5 mm. The dosimetric planning was performed prior to the procedure. A dose of 100 Gy at 7 mm depth was prescribed after calculating the dose rate according to the current activity of the source. The scleral dose was 929 Gy. The duration of the application was 166.7 hours (almost 7 days).
After taking necessary consent and ensuring sterility and radiation safety, the patient was posted for the procedure under general anaesthesia. The eyelid was retracted, and a tunnel was made to position the dummy source, on the scleral surface above the tumour (Figure 2). Indirect fundoscopy was done to confirm the tumour location. The dummy source was then removed. The radioactive plaque was gently applied over the area of bare sclera adjacent to the limbus and sutured (Figure 3). The final position of the plaque was again confirmed with indirect fundoscopy (Figure 4). During the entire treatment, lubricants and other eye drops were used as needed. Radiation safety during the entire procedure was ensured with the use of handheld radiation counters and wipe tests for all surgical instruments to rule out leakage of radiation. All healthcare personnel were required to wear thermoluminescent dosimeter (TLD) badges during the procedure. After the plaque placement, the eye was patched, and the patient was shifted to an isolation room. The attendants were advised to maintain a distance of at least 6 feet from the patient as a precautionary measure. The plaque was removed under local anaesthesia after the completion of the calculated time. There was mild conjunctival and scleral congestion with no other major problems. The patient was discharged, and his first follow-up after 3 months is awaited.
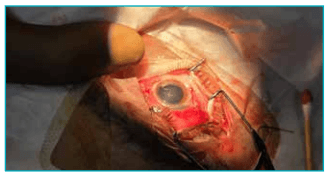
Figure 2: Retraction of the eyelid for the placement of the plaque.
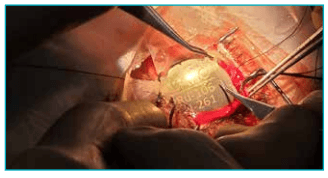
Figure 3: Placement of the radioactive plaque.
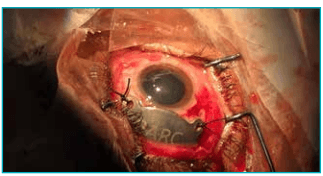
Figure 4: Final positioning of the plaque.
Discussion
Plaque brachytherapy is a form of localised internal radiation therapy widely used in ophthalmic oncology to treat intraocular tumours such as uveal melanoma, retinoblastoma, and certain benign tumours (e.g., circumscribed choroidal haemangioma). Among various radionuclide plaques, ¹⁰⁶Ru has become a commonly employed isotope due to its favourable dosimetric and clinical properties. Unlike external beam radiation, plaque brachytherapy provides high doses to the tumour while sparing adjacent critical structures like the optic nerve and macula.5
In India, the Bhabha Atomic Research Centre (BARC) has developed indigenous plaques, making them more cost-effective. Two types of plaques are commercially available – notch and round. They vary slightly in their dose distribution parameters, while the basic principle for both remains the same. Round plaques can be used for treating slightly larger tumours, while notch plaque is used for smaller or posteriorly located tumours where optic nerve shielding is needed. Essentially, the plaque is made up of three silver layers: a 15.8 mm diameter and 0.9 mm thick backing plate, a 13.3 mm diameter and 0.2 mm thick silver substrate that contains 106Ru, and a 0.1 mm thick silver window. Both these plaques are available for treatment with our department. Considering the larger tumour size, our patient was treated with the round plaque.6
Over decades, retrospective studies and meta-analyses have provided data on efficacy, local control, survival, and toxicity profiles of ¹⁰⁶Ru plaques. ¹⁰⁶Ru is a pure beta emitter with a maximum energy of approximately 3.5 MeV. Its emissions result in a steep dose fall-off beyond a few millimetres, delivering a high radiation dose at the plaque surface but quickly reducing energy deposition in deeper tissues. This characteristic is advantageous for treating superficial or moderately deep tumours while limiting exposure to deeper ocular structures such as the retina and lens. However, its limited penetration makes it less effective for thicker tumours (> 7–8 mm), where other isotopes like 125I may be preferred. For treatment purposes, tumour thickness is calculated as the height of the tumour along with the scleral thickness. The tumour thickness calculated in this case was 9 mm. We plan to assess the response to therapy at 3–6 months from completion of treatment and plan further local therapy in case of any residual disease. This is a widely accepted treatment technique considering the logistics related to radioactive plaque availability.4
Plaque brachytherapy with ruthenium involves scleral fixation of a plaque directly adjacent to the tumour base. The desired delivered radiation dose to the tumour apex usually ranges from 70 Gy to > 140 Gy, depending on tumour characteristics and institutional protocols. We treated our patient with a total dose of 100 Gy as per the recommendation for the primary treatment of choroidal melanomas.5The shorter range of beta emission translates to lower radiation exposure of nearby normal tissues compared with gamma-emitting sources and subsequently easier handling of the radioactive source. The closest nearby normal tissue of concern in our patient was the sclera. The tumour was away from the optic nerve. The decision regarding total treatment dose is guided by acceptable scleral doses to prevent related toxicity. In ¹⁰⁶Ru plaque brachytherapy, the sclera inevitably receives very high radiation doses because the plaque is sutured directly onto the episcleral surface and ¹⁰⁶Ru is a beta emitter with a steep dose fall-off. The sclera is a radio-resistant structure, and scleral surface doses typically range from 400 to 1500 Gy, and in some series may exceed 2000 Gy, particularly for thicker tumours where a therapeutic apex dose (70–100 Gy) is prescribed. The spectrum of scleral toxicity can vary from scleritis to necrosis and subsequent vision loss. Despite these high doses, clinically significant scleral necrosis is uncommon, with reported rates generally below 5% in large series.7
Uveal melanoma is the most common primary intraocular malignant tumour in adults. In terms of survival with plaque treatment, an institutional report from MD Anderson showed extremely high 5-year control (97%) and overall survival (92%) in 40 uveal melanoma patients treated with ¹⁰⁶Ru plaques, with low rates of enucleation and acceptable toxicity.7
A meta-analysis of 21 studies involving nearly 4000 patients with uveal melanoma treated with plaque brachytherapy showed local control rates ranging from approximately 59% to 98%. Larger tumours had lower local control rates. The most commonly reported complications were cataract and radiation-related retinopathy. This metaanalysis established that 106Ru brachytherapy seems to be successful in achieving local control of uveal melanoma.5
Studies comparing ¹⁰⁶Ru brachytherapy with enucleation in thicker tumours (apex ≥ 8 mm) reported similar melanomarelated mortality between plaque therapy and enucleation, with eye preservation achieved in over 70% of cases.8
Conclusion:
Plaque brachytherapy is an established first-line curative treatment modality in multiple ocular tumours. Establishing a plaque brachytherapy facility is challenging and time- and resource-consuming. It also needs a motivated multidisciplinary team to make it a successful programme. There is a learning curve to it, and adequately trained manpower is one of the cornerstones in having a successful plaque brachytherapy service.
Dodul Mondal, Vrinda Singla, Sobhana VVVS, Anita Sethi, Nikhil Pal. Saving the Sight: Expanding the
Therapeutic Horizon in Ophthalmic Tumours and Successful Introduction of Plaque Brachytherapy at
Max Super Speciality Hospital, Saket. MMJ. 2026, March. Vol 3 (1).
References
- Belaïd A, Nasr C, Jmour O, et al. Brachytherapy of Uveal Melanomas with Ruthenium-106 Plaques. Asian Pac J Cancer Prev. 2016;17(12):5281–5.
- Cennamo G, Montorio D, D’ Andrea L, et al. Long-Term Outcomes in Uveal Melanoma After Ruthenium-106 Brachytherapy. Front Oncol. 2022;11:754108.
- Thomas GN, Chou IL, Gopal L. Plaque Radiotherapy for Ocular Melanoma. Cancers (Basel). 2024;16(19):3386.
- Thomson RM, Furutani KM, Kaulich TW, et al. AAPM recommendations on medical physics practices for ocular plaque brachytherapy: Report of task group 221. Medical Physics. 2020;47(5):e92–124.
- Karimi S, Arabi A, Siavashpour Z, et al. Efficacy and complications of ruthenium-106 brachytherapy for uveal melanoma: a systematic review and meta-analysis. J Contemp Brachytherapy. 2021;13(3):358–64.
- Kumar R, Srivastava A, Kakade N, et al. Dosimetry of indigenously developed 106Ru-106Rh ophthalmic plaque. Brachytherapy. 2024;23(4):443–56.
- Takiar V, Gombos DS, Mourtada F, et al. Disease control and toxicity outcomes using ruthenium eye plaque brachytherapy in the treatment of uveal melanoma. Pract Radiat Oncol. 2014;4(4):e189–94.
- Kaiserman N, Kaiserman I, Hendler K, et al. Ruthenium-106 plaque brachytherapy for thick posterior uveal melanomas. Br J Ophthalmol. 2009;93(9):1167–71.