

Abstract:
Traumatic tracheobronchial injury often necessitates surgical intervention when complicated by airway disruption. If not managed properly and timely, it can lead to significant morbidity and mortality. Clinical manifestations of tracheobronchial injury include persistent pneumothorax, subcutaneous emphysema, pneumomediastinum, and respiratory insufficiency. Bronchoplasty using a pericardial patch is a rare but crucial surgical technique aimed at restoring bronchial integrity to preserve pulmonary function. This case report discusses the successful anaesthetic management of a patient who underwent left-sided bronchoplasty using a pericardial patch for traumatic bronchial fracture reconstruction. The anaesthetic challenges in this case were the paediatric age group of the patient, compromised gas exchange due to complete left lung collapse, requirement of differential one-lung ventilation (OLV) to provide an optimal surgical field to the surgeon, maintenance of gas exchange and haemodynamic stability intraoperatively, and to ensure bronchial suture integrity to reduce the risk of air leaks postoperatively. A right-sided double-lumen tube (DLT) with pressure-controlled ventilation was used for differential right lung ventilation, strict haemodynamic monitoring, and multimodal analgesia. The patient was extubated postoperatively to avoid barotrauma and bronchial suture disruption. A multidisciplinary approach with vigilant airway management, lung-protective ventilation strategies, and postoperative care is essential for optimal outcomes in these patients.
Key words: Paediatric Anaesthesia, Traumatic Bronchial Injury, Bronchoplasty, One-Lung Ventilation, DoubleLumen Tube, Thoracic Anaesthesia.
Introduction
Tracheobronchial injury (TBI) is a rare incidence following blunt chest trauma and can often be missed. Traumatic bronchial injury is estimated to occur in 2%–3% of patients who succumb to traumatic injury.1,2 Blunt trauma has a lower incidence of TBI (0.5%–2%) as compared to penetrating trauma (1%–2%).2
It requires a high level of suspicion for timely diagnosis and proper treatment, failure of which can lead to significant morbidity and mortality. Diagnosis is confirmed by fibreoptic bronchoscopy or by computed tomography (CT) of the chest. Complex injuries involving bronchial rupture may require pneumonectomy in many cases. Bronchoplasty can be used as a lung-sparing surgical approach for airway reconstruction in these cases and presents unique perioperative anaesthetic challenges, such as management of perioperative airway, ventilation, perfusion, providing an optimal surgical field to surgeons, and postoperative care. The preferred airway management technique is to intubate the healthy bronchus with either a single-lumen tube or a double-lumen tube (DLT).3,4
Deceleration injury resulting from blunt chest trauma commonly occurs at the transition zone between the fixed and mobile bronchus within 2.5 cm of the carina. These injuries are more common on the right side and 10 times more common in adults due to their hard bone contour as compared to the pliable chest wall in children.4 This case report discusses the successful anaesthetic management of a 14-year-old male child who underwent left thoracotomy and bronchoplasty using a bovine pericardial patch for traumatic left bronchial fracture– stenosis resulting in complete left lung collapse. A rightsided DLT was used for differential lung ventilation.
Case Report
A 14-year-old male patient presented to the emergency department with complaints of difficulty in breathing, left-sided chest pain, and a history of blunt chest trauma 2 weeks earlier. Auscultation revealed absent air entry on the left side, and a left-sided intercostal drain (ICD) in situ. The patient had previously been admitted to another hospital after trauma with the same complaints, where fibreoptic bronchoscopy (FOB) was attempted but had to be abandoned due to the development of tachycardia and hypoxia. ICD was placed on the left side for pneumothorax; however, persistent symptoms prompted referral for definitive treatment.
Preoperative evaluation revealed a heart rate (HR) of 135 beats/min, blood pressure (BP) of 112/78 mmHg, oxygen saturation (SpO2) of 96% on 2 L of oxygen (02) via nasal prongs, respiratory rate (RR) of 20 breaths/ min, weight of 45 kg, height of 142 cm, and absent air entry to the left side of the chest on auscultation. Blood investigations were all within normal limits. Chest X-ray revealed a completely collapsed left lung with ipsilateral volume loss and shift, giving clinical suspicion of endobronchial injury (Figure 1A). Contrast-enhanced computed tomography (CECT) of the thorax revealed a complete cut-off of the left main bronchus, indicative of traumatic bronchial disruption (Figure 1B). Flexible bronchoscopy confirmed the absence of a bronchial lumen 2.8 cm from the carina on the left, supporting the diagnosis of complete bronchial transection (Figure 2).

Figure 1: A. Chest radiograph showing complete collapse of the left lung with ipsilateral volume loss and mediastinal shift; B. Contrast-enhanced computed tomography (CECT) of the thorax revealing complete cut-off of the left main bronchus, consistent with traumatic bronchial disruption.
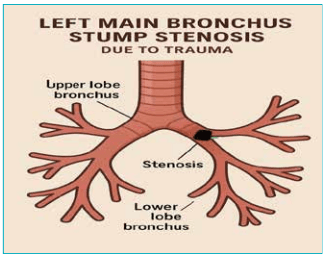
Figure 2: Schematic representation showing complete obliteration of the left main bronchus approximately 2.8 cm distal to the carina, confirming traumatic bronchial transection.
Intraoperative anaesthetic management
In the operating room, monitors were attached, and two wide-bore intravenous cannulae were secured. Patient was preoxygenated and premedicated with glycopyrrolate, midazolam, and fentanyl. Anaesthesia was induced with propofol, and the muscle relaxant atracurium was administered. The patient was intubated with a rightsided 35 Fr DLT, and correct positioning was confirmed through fibreoptic bronchoscopy. One-lung ventilation (OLV) of the right side was achieved after blocking the tracheal lumen. The patient was ventilated on pressurecontrol mode, keeping peak airway pressures between 25–28 mmHg and positive end-expiratory pressure (PEEP) of 5 cmH2O, to attain a tidal volume of approximately 350 mL and a respiratory rate of 18 breaths/min. Endtidal carbon dioxide (ETCO2) was maintained between 35–40 mmHg, and SpO2 remained at 94%–96% on 0.5 FiO2. The right radial artery was cannulated for continuous blood pressure monitoring and blood gases measurement. Anaesthesia was maintained with sevoflurane, oxygen and air. Paracetamol, diclofenac, and morphine were given as analgesics. Surgery was conducted in the right lateral position. Haemodynamics were maintained throughout the surgery within normal limits.
Intraoperatively, the left main bronchus was found to be fractured, fibrosed, and stenosed, causing obliteration of the distal bronchial segment with total lung collapse, which was repaired with a bovine pericardial patch.
After bronchoplasty, the tracheal lumen was declamped to allow both lungs to inflate and check for leaks from the anastomotic site. No air leak was found, and the left lung was slowly inflated. The patient maintained saturation of 98% on pressure-control ventilation. The thoracotomy was closed after insertion of an ICD.
The patient was reversed and extubated after confirming adequate respiratory efforts. Postoperatively, he was kept on spontaneous ventilation to avoid barotrauma and prevent suture disruption.
Postoperative care
The patient was shifted to the Intensive Care Unit (ICU) for further observation. Vital parameters were maintained, with SpO2 of 98% on 4 L/min of 02 via mask. Multimodal analgesia was used with paracetamol, non-steroidal anti-inflammatory drugs (NSAIDS), and morphine. On postoperative Day 1, the patient was ambulated, deep breathing exercises were encouraged, and spirometry was done thrice a day. There were no postoperative complications. By the postoperative Day 7, chest X-ray revealed re-expansion of the left lung, mediastinal normalisation, and no evidence of anastomotic leak or stricture (Figure 3). ICD was removed, and the patient was discharged in a stable condition with good pulmonary function.
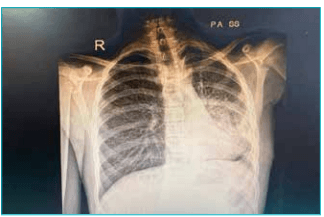
Figure 3: Postoperative chest radiograph demonstrating reexpansion of the left lung with normalisation of mediastinal position and no evidence of air leak, anastomotic disruption, or residual bronchial stenosis.
Discussion
Anaesthetic management in thoracic trauma with bronchial injury is complex and multifaceted. Traumatic tracheobronchial injury often necessitates surgical intervention when complicated by airway disruption. If not managed properly and timely, it can lead to significant morbidity and mortality.3 Diagnosis in these patients can be difficult, which may cause a delay in treatment.5 Presentation of unexplained dyspnoea, recurrent pneumonia and unresolved pneumothorax, even with ICD in a patient with a previous history of trauma, should raise suspicion of missed bronchial injury.6 Bronchoplasty using a pericardial patch is a rare but crucial surgical technique aimed at restoring bronchial integrity to preserve pulmonary function.
The key challenge in these patients is achieving adequate oxygenation and ventilation during OLV. Maintaining low airway pressures is vital to protect suture lines and pericardial patch integrity. Recommended methods for securing the airway in patients with tracheobronchial injury include DLT, bronchial blockers, single-lumen Endotracheale tube (ETT).
Bronchial blockers are easier to displace and provide limited suction and drainage to the isolated lung, leading to accumulation of pus, blood or secretions. It can also interfere with the surgical field since they are placed in the operative bronchus. Management with a single-lumen ETT with positive pressure ventilation is likely to cause air leakage and produce further deterioration of pulmonary function.4 The use of a DLT confirmed by bronchoscopy is the gold standard for OLV. Previous studies have also supported the use of high-frequency jet ventilation if OLV fails. A right-sided DLT with pressure-control mode was used for differential right lung ventilation. Strict haemodynamic monitoring was done, multimodal analgesia was used intraoperatively, and the patient was extubated postoperatively to avoid any barotrauma and bronchial suture disruption by elective ventilation.
Protective ventilation strategies are crucial in avoiding further lung damage. Injury from OLV can cause reexpansion pulmonary oedema (REPE), acute lung injury (ALI), or acute respiratory distress syndrome (ARDS). Early ALI is predicted by high intraoperative ventilation pressures. Reduction of tidal volumes during OLV to 5 mL/kg has been shown to reduce alveolar concentration of tumour necrosis factor (TNF) and soluble intercellular adhesion molecule-1 (sICAM-1). However, fixed volumes of 9 mL/kg with the addition of 5 cmH2O PEEP was associated with better oxygenation and earlier extubation.5
Pain control promotes pulmonary recovery. Postoperative ICU care is essential for the timely diagnosis and management of complications such as bronchopleural fistula, ARDS, and persistent air leak. If the patient is haemodynamically unstable and requires postoperative ventilation, it should be done with low tidal volume.
Multidisciplinary coordination among anaesthesiologists, thoracic surgeons, and intensivists significantly improves outcomes in such high-risk procedures.
Conclusion:
Anaesthesia for thoracotomy with bronchoplasty in a patient with bronchial injury demands meticulous airway planning, lung-protective ventilation, and vigilant perioperative monitoring. Personalised ventilation strategies and adequate analgesia play pivotal roles in reducing morbidity. A well-orchestrated team of a surgeon, anaesthesiologist and pulmonologist enhances safety and facilitates recovery.
Kavya Gangwar, Hricha Bhandari, Arun Puri. Anaesthetic Considerations in a
Paediatric Patient Posted for Left Pericardial Patch Bronchoplasty for Traumatic Left
Main Bronchus Fracture–Stricture. MMJ. 2026, March. Vol 3 (1).
References
- Kaptanoglu M, Dogan K, Nadir A, et al. Tracheobronchial rupture: a considerable risk for young teenagers. Int J Pediatr Otorhinolaryngol. 2002;62:123–8.
- Rossbach MM, Johnson SB, Gomez MA, et al. Management of major tracheobronchial injuries: a 28-year experience. Ann Thorac Surg. 1998;65:182–6.
- Miller RD, Cohen NH, Eriksson LI, et al. Miller’s Anesthesia. 9th Edition. Elsevier; 2020.
- Hosalli V, Ambi US, Ganeshnavar A, et al. Anaesthetic considerations in primary repair of tracheobronchial injury following blunt chest trauma in paediatric age group: experience of two cases. Indian J Anaesth. 2013;57:410–2.
- Tsai J, Moon T, Vachhani S, et al. Anesthesia for thoracic surgical procedures. In: Firstenberg MS, ed. Principles and Practice of Cardiothoracic Surgery. InTech; 2013.
- Anjum S, Reema M, Vyas CK. Anaesthetic management of primary repair of complete right bronchial rupture following blunt chest trauma. Egypt J Cardiothorac Anesth. 2015;9(3):46–8.