

Abstract:
Osteoarthritis (OA) is a highly prevalent musculoskeletal disorder causing chronic pain and disability. As many patients fail conservative therapy or are unsuitable for surgery, effective non-invasive options are needed. Low-dose radiation therapy (LDRT) has re-emerged as a treatment targeting OA-related inflammation and providing symptom relief. This narrative review summarises the epidemiology and pathophysiology of OA, the radiobiological rationale for LDRT, patient selection criteria, clinical outcomes, and safety considerations. Evidence from randomised controlled trials, observational studies, and international guidelines — particularly German Society for Radiation Oncology (DEGRO) — was also reviewed. At low doses (0.5–1.0 Gy per fraction; total 3 Gy), LDRT exerts anti-inflammatory effects that translate into significant pain relief and functional improvement in OA of affected joints. Evidence from randomised and observational studies showed good tolerance, mild to no toxicity, and an extremely low theoretical risk of secondary malignancy. DEGRO guidelines endorse LDRT as an adjunctive treatment for selected patients with painful OA who have failed conservative therapy or are unsuitable for surgery. LDRT is a safe, evidence-based, non-invasive option that provides effective pain relief and functional improvement in selected patients with osteoarthritis. By addressing chronic joint inflammation, it offers a practical therapeutic “middle ground” between conservative management and surgery. Further research is warranted to optimise patient selection, timing, and predictive biomarkers of response.
Key words: Osteoarthritis, Low-Dose Radiation Therapy, Pain Relief.
Introduction
Osteoarthritis (OA) affects nearly 595 million people globally and is a leading cause of pain and disability. By 2050, OA prevalence is projected to increase by 74.9% for the knee, 48.6% for the hand, 78.6% for the hips, and 95.1% for other joints. 1 In India, symptomatic OA cases rose 2.66-fold, from 23.46 million in 1990 to 62.3 million in 2019. 2 OA is no longer viewed as a simple “wear-and-tear” disorder but as a disease of joint failure, involving cartilage degeneration and chronic low-grade inflammation. 3 OA risk increases with age and is influenced by female sex, obesity, prior injury, and genetic factors. While management ranges from lifestyle measures and pharmacotherapy to surgery, a subset of patients remains refractory to conservative treatment, yet unsuitable or unwilling for surgical intervention. For such patients, low-dose radiation therapy (LDRT) offers a non-invasive, effective therapeutic option, addressing the inflammatory component of OA. 3
Historical Perspective
The use of radiation for non-malignant diseases dates back nearly a century. Following the discovery of X-rays by Wilhelm Conrad Röntgen in 1895 and radioactivity by Henri Becquerel and Marie Curie, radiotherapy was rapidly adopted for a wide range of benign conditions, often without robust evidence or long-term safety data. 4 As early as 1898, X-rays were reported to provide effective pain relief in patients with arthritis. 5 However, growing recognition of the risk of radiation-induced secondary malignancies led to fear and uncertainty, resulting in a gradual global decline in the use of radiotherapy for benign diseases.
Radiobiological Rationale for LDRT
LDRT exerts anti-inflammatory and immunomodulatory effects that result in pain relief (Figure 1). At doses used for OA (0.3–1.0 Gy), 6 LDRT downregulates pro-inflammatory cytokines (tumour necrosis factor-α [TNF-α], interleukin-1β [IL-1β], interleukin-6 [IL-6]), upregulates anti-inflammatory mediators (transforming growth factor-β [TGF-β]), reduces endothelial activation and leukocyte recruitment, and promotes macrophage polarisation towards an antiinflammatory (M2) phenotype. 7 These combined effects suppress chronic synovial inflammation and nociceptive signalling, leading to improved pain and joint function without significant structural damage. 8
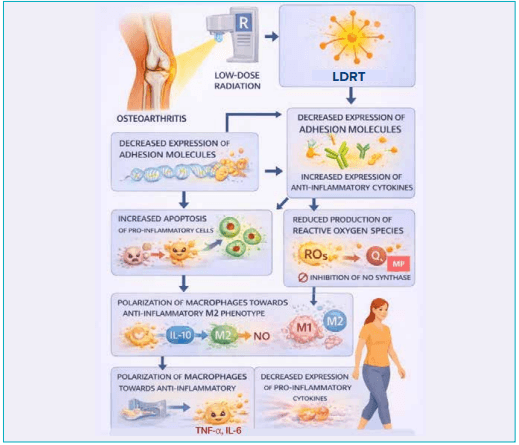
Figure 1: Radiobiological mechanisms of the anti-inflammatory effect of low-dose radiation therapy4
Abbreviations: DNA: Deoxyribonucleic Acid; IL-6: Interleukin-6; IL-10: Interleukin-10; LDRT: Low-Dose Radiation Therapy; M1: Classically Activated Macrophages; M2: Alternatively Activated Macrophages; MP: Metalloproteinases; NO: Nitric Oxide; O4: Tetraoxygen; ROS: Reactive Oxygen Species; TNF-α: Tumour Necrosis Factor-α.
Indications and Contraindications for LDRT in OA
Appropriate patient selection for LDRT in OA is essential, as it plays a key role in determining the treatment outcomes shown in Table 1.
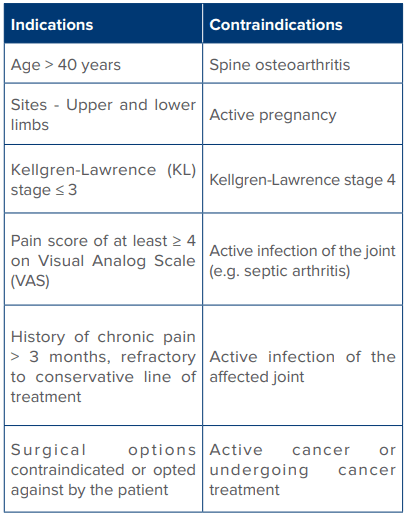
Table 1 : Indications and contraindications of low-dose radiation therapy for osteoarthritis.4
Treatment Planning
LDRT planning involves patient consent, computed tomography (CT) simulation with immobilisation, and target volume delineation, with careful shielding of adjacent critical structures (Figures 2, 3A and 3B). Based on clinical studies and international guidelines, the standard dose for OA is 3 Gy in 6 fractions (0.5 Gy each) over 2 weeks. 9 Treatment response is assessed at 6–8 weeks using the Visual Analogue Scale (VAS), Numeric Rating Scale (NRS), or Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores. 10,11 In cases of partial or no response, a second LDRT course may be delivered 8–12 weeks after the initial treatment.12,13
Risk-Benefit Profile
Benefits of LDRT for OA:
- Reduction in pain, improvement in joint function and improved quality of life
- Non-invasive treatment option
- Minimal to no acute toxicity and good overall tolerance
- Potential benefit in patients with refractory OA who have failed conservative therapies
- Long-term effect
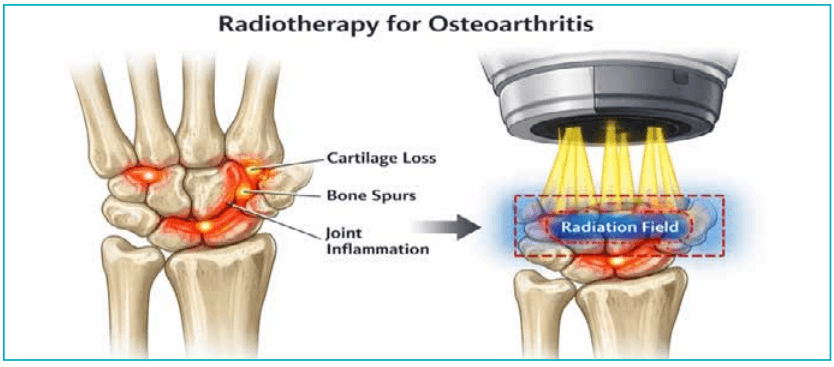
Figure 2: Graphic representation of a wrist joint showing changes of osteoarthritis. Only the affected area is targeted as per guidelines and treated with low-dose radiation therapy.
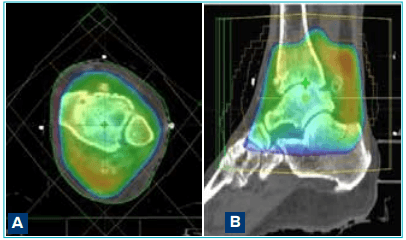
Figure 3A and B: Computed tomography-based target delineation and dose distribution for ankle osteoarthritis.
Risks of LDRT for OA:
- Acute (early) toxicities (< 1%). A small but non-negligible theoretical risk of radiation-induced malignancy has been described; however, contemporary evidence suggests this risk is extremely low when low-dose regimens and appropriate patient selection are employed. 13
LDRT for OA in Randomised Trials and Guidelines
Some randomised trials exist in the literature, highlighting the promising role of LDRT for OA, as shown in Table 2.
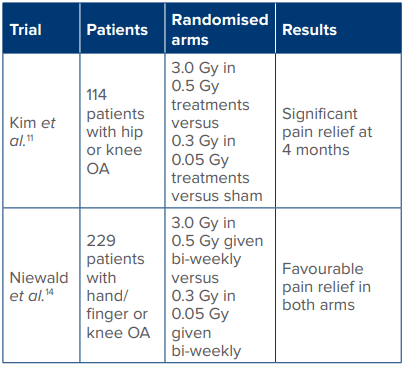
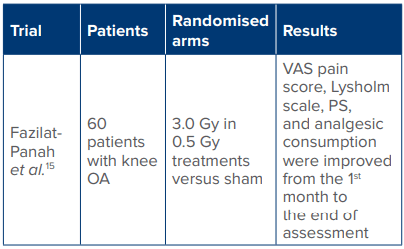
Table 2 : Randomised trials highlighting the successful role of low-dose radiation therapy in osteoarthritis.
Abbreviations: Gy: Gray; OA: Osteoarthritis; PS: Pain Score; VAS: Visual Analogue Scale.
Few case series and observational studies are mentioned in Table 3.
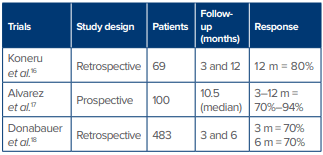
Table 3: Case series and observational studies highlighting the role of low-dose radiation therapy in osteoarthritis.
DEGRO guidelines:
These comprehensive guidelines by the German Society for Radiation Oncology support the use of LDRT as a non-invasive, adjunctive option for painful OA, and are summarised below (Table 4). 9
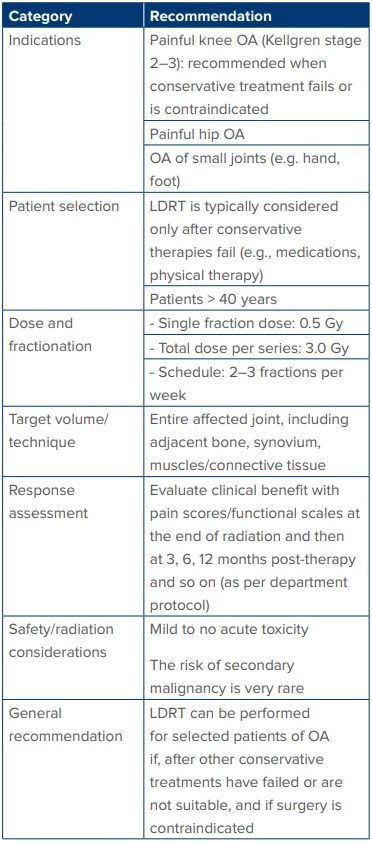
Table 4: Summary of the German Society for Radiation Oncology (DEGRO) guidelines for use of LDRT in OA.
Abbreviations: LDRT: Low-Dose Radiation Therapy; Gy: Gray; OA: Osteoarthritis; RT: Radiotherapy.
A summary of common queries and their evidence-based responses are mentioned in Table 5.
Future Directions
Given the rising global burden of OA, LDRT offers a valuable non-surgical option for pain relief, supported by four randomised trials and multiple case series showing significant benefits. Future research should refine timing, predictive inflammatory markers, concurrent therapies, and site-specific efficacy.
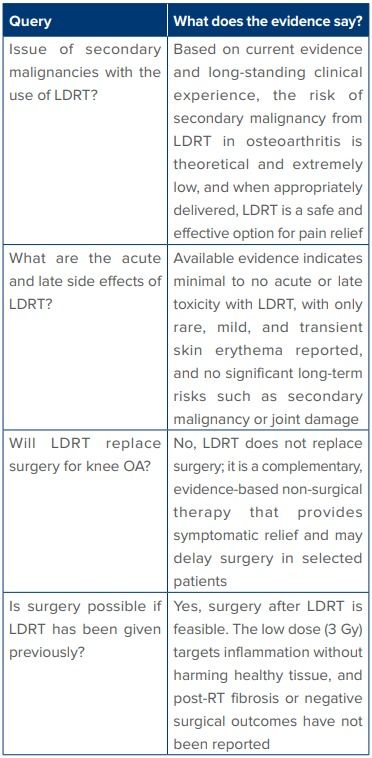
Table 5: Queries and concerns about LDRT
Abbreviations: LDRT: Low-Dose Radiation Therapy; Gy: Gray; OA: Osteoarthritis; RT: Radiotherapy
Conclusion:
As evidence continues to evolve, LDRT could emerge as a practical “middle-ground” treatment for osteoarthritis, offering an effective bridge between conservative management and surgical intervention.
Khushboo Rastogi, Nidhi Sharma, Varshu Goel, Garima Singh, Anusheel Munshi. Revisiting Radiotherapy:
Low-Dose Radiation Therapy for Refractory Osteoarthritis. MMJ. 2026, March. Vol 3 (1).
References
- GBD 2021 Osteoarthritis Collaborators. Global, regional, and national burden of osteoarthritis, 1990–2020 and projections to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023;5(9):e508–22.
- Singh A, Das S, Chopra A, et al. Burden of osteoarthritis in India and its states, 1990–2019: findings from the Global Burden of Disease Study 2019. Osteoarthritis and Cartil. 2022;30(8):1070–8.
- Tang S, Zhang C, Oo WM, et al. Osteoarthritis. Nat Rev Dis Primers. 2025;11(1):10.
- Fletcher GH. Regaud lecture perspectives on the history of radiotherapy. Radiother Oncol. 1988;12:253–71.
- Sokoloff N. Roentgenstrahlen gegen Gelenkrheumatismus. Fortschr Rontgenstr. 1898;209 –13.
- Rödel F, Keilholz L, Herrmann M, et al. Radiobiological mechanisms in inflammatory diseases of low-dose radiation therapy. Int J Radiat Biol. 2007;83(6):357–66.
- van den Bosch MHJ, van Lent PLEM, van der Kraan PM. Identifying effector molecules, cells and cytokines of innate immunity in OA. Osteoarthr Cartilage. 2020;28(5):532–43
- Dove, Austin OH, et al. The Use of Low-Dose Radiation Therapy in Osteoarthritis: A Review. Int J Rad Oncol Biol Phy. 2022;114(2):203–20.
- Ott OJ, Niewald M, Weitmann HD, et al. DEGRO guidelines for the radiotherapy of non-malignant disorders. Strahlenther Onkol. 2014;191(1):1–6.
- Rühle A, Tkotsch E, Rainer Mravlag, et al. Low-dose radiotherapy for painful osteoarthritis of the elderly: A multicenter analysis of 970 patients with 1185 treated sites. Strahlenther Onkol. 2021;197(10):895–902.
- Kim BH, Shin K, Kim MJ, et al. Low-dose RaDiation therapy for patients with KNee osteoArthritis (LoRD-KNeA): a protocol for a sham-controlled randomised trial. BMJ Open. 2023;13(2):e069691.
- Rogers S, Eberle B, Vogt DR, et al. Prospective Evaluation of Changes in Pain Levels, Quality of Life and Functionality After Low Dose Radiotherapy for Epicondylitis, Plantar Fasciitis, and Finger Osteoarthritis. Front Med. 2020:7:195.
- Schlamann A, Yu J, Ruhle A. Low-Dose Radiotherapy for Osteoarthritis: Current Evidence, Practical Recommendations and Future Perspectives. Semin Radiat Oncol. 2026;36:39–47.
- Niewald M, Müller LN, Hautmann MG, et al. ArthroRad trial: multicentric prospective and randomized single-blinded trial on the effect of low-dose radiotherapy for painful osteoarthritis depending on the dose-results after 3 months' follow-up. Strahlenther Onkol. 2022;198(4):370–7.
- Fazilat-Panah D, Javadinia SA, Shabestani Monfared A, et al. Effects of low dose rate radiotherapy on pain relief, performance score, and quality of life in patients with knee osteoarthritis; a double-blind sham-controlled randomized clinical trial. Int J Radiat Biol. 2025;101(5):541–8.
- Koneru BN, Sick J, Shaikh HA, et al. Low-Dose Radiation Therapy for Osteoarthritis: A Retrospective Single-Institution Analysis of 69 Patients and 168 Joints. Int J Radiat Oncol Biol Phys. 2025;123(2):352–60.
- Álvarez B, Montero A, Alonso R, et al. Low-dose radiation therapy for hand osteoarthritis: shaking hands again? Clin Transl Oncol. 2022;24(3):532–9.
- Donaubauer AJ, Zhou JG, Ott OJ, et al. Low Dose Radiation Therapy, Particularly with 0.5 Gy, Improves Pain in Degenerative Joint Disease of the Fingers: Results of a Retrospective Analysis. Int J Mol Sci. 2020;21(16):5854