

Abstract:
Implant-based breast reconstruction following nipple-sparing mastectomy (NSM) has gained increasing acceptance due to its oncological safety and favourable aesthetic outcomes. It can be performed in immediate or delayed settings depending on disease biology and patient factors. We present a two-patient case series from a dedicated breast unit. The first patient underwent bilateral NSM with immediate implant-based reconstruction for synchronous bilateral breast carcinoma. The second patient, with Li-Fraumeni syndrome, underwent interval NSM and reconstruction following prior breast-conserving surgery and chemotherapy. Surgical technique, perioperative outcomes, and early aesthetic results were evaluated. Both patients underwent successful subpectoral silicone implant placement with native acellular dermal matrix (ADM) support. No intraoperative or postoperative complications were observed. Nipple–areola complex (NAC) viability was preserved in both cases. Patients demonstrated satisfactory wound healing, early mobilisation, and favourable aesthetic outcomes at follow-up. Implant-based reconstruction following NSM is a safe and effective option in carefully selected patients. Both immediate and interval reconstructions can be performed with excellent clinical and aesthetic outcomes in a multidisciplinary setting.
Key words: Breast Cancer, Implant-Based Reconstruction, Nipple-Sparing Mastectomy, Immediate Reconstruction, Interval Reconstruction, Acellular Dermal Matrix.
Introduction
Breast reconstruction has become an essential component of comprehensive breast cancer care, with a significant impact on psychological well-being, body image, and quality of life. Implant-based reconstruction is currently the most performed reconstructive modality worldwide, owing to its shorter operative time, reduced donor site morbidity, and predictable outcomes compared to autologous reconstruction.1
Nipple-sparing mastectomy (NSM) represents an evolution in surgical management, preserving the nipple–areola complex (NAC) while achieving oncological safety in appropriately selected patients. Multiple studies have demonstrated that NSM does not compromise oncological outcomes when careful patient selection criteria are followed, including tumour size, location, and absence of NAC involvement.2,3
Immediate breast reconstruction offers psychological benefits and reduces the number of surgical procedures, while delayed or interval reconstruction remains valuable in patients requiring staged oncologic treatment, genetic risk evaluation, or contraindications to immediate reconstruction.4
The use of acellular dermal matrix (ADM) has further improved implant-based reconstruction by providing additional soft tissue support, improved implant positioning, and enhanced aesthetic outcomes.5
This case series aims to highlight the feasibility and safety of implant-based reconstruction following NSM in two distinct clinical scenarios — immediate bilateral reconstruction and interval unilateral reconstruction in a patient with Li-Fraumeni syndrome — demonstrating versatility across varied oncological contexts.
Methods
This is a retrospective case series of two patients undergoing implant-based breast reconstruction following nipple-sparing mastectomy at a tertiary care breast unit. Both patients were evaluated in a multidisciplinary tumour board. Surgical planning was individualised based on tumour characteristics, genetic profile, and patient preference.
Outcomes assessed included:
- Operative details
- Postoperative recovery
- Complications
- Early aesthetic outcomes
Case Report
Case report 1: Immediate bilateral implant-based reconstruction
A 44-year-old female presented with synchronous bilateral breast malignancy. Clinical examination revealed a 3 × 2 cm lesion in the left breast and a 1.5 × 1.5 cm lesion in the right axillary tail. Imaging, including mammography, magnetic resonance imaging (MRI), and positron emission tomography-computed tomography (PET-CT), confirmed localised disease without distant metastasis.
Histopathology demonstrated invasive breast carcinoma of no special type (IBC-NST) — Grade 1, luminal A subtype; oestrogen receptor/progesterone receptor (ER/PR) positive, human epidermal growth factor receptor 2 (HER2) negative, Ki-67 4%–5%. Genetic testing was negative for breast cancer gene (BRCA) mutations.
The patient underwent bilateral NSM with a sentinel lymph node biopsy. The left sentinel lymph node was positive (1/4 nodes), necessitating complete axillary lymph node dissection (levels I–II). Important neurovascular structures, including the thoracodorsal pedicle and long thoracic nerve, were preserved.
Reconstruction was performed immediately using subpectoral silicone implants (320 cc with a moderate profile) with native ADM support. A hockey-stick incision was used bilaterally, and well-vascularised skin flaps were raised while preserving NAC vascularity. The mastectomy specimen weights were 318 g (left) and 354 g (right).
A subpectoral pocket was created, and ADM was sutured inferolaterally to create a sling. Closed suction drains were placed, and wounds were closed in layers.
The postoperative course was uneventful. The patient was mobilised on the same day and discharged on postoperative Day 2 with healthy wounds and preserved NAC viability.
Case report 2: Interval unilateral implant-based reconstruction
A 27-year-old female with carcinoma of the left breast in the background of Li-Fraumeni syndrome (TP53 mutation positive) had previously undergone breast-conserving surgery, sentinel lymph node biopsy, and chemotherapy. Initial histopathology revealed invasive carcinoma (Grade III) with ductal carcinoma in situ (DCIS) — ER 2/8, PR 4/8, HER2 negative, Ki-67 55%. Final staging was pT1cN0.
Given the genetic predisposition and contraindication to radiotherapy, definitive surgical management with mastectomy was planned.
The patient underwent left NSM via a lateral mammary crease incision. A well-vascularised skin flap was raised while preserving NAC. The mastectomy specimen weighed 460 g.
Reconstruction was performed using a 390 cc moderate profile silicone implant placed in a subpectoral pocket with native ADM support. The ADM was secured inferolaterally to create a sling, and a closed suction drain was placed.
The postoperative course was uneventful, with early mobilisation and good wound healing. The patient was discharged on postoperative Day 1 with a satisfactory aesthetic outcome and preserved NAC viability.
Results
Both patients underwent successful implant-based reconstruction without intraoperative complications (Table 1)
- No surgical site infection, haematoma, or seroma was observed
- NAC viability was preserved in both cases
- Hospital stay was 1–2 days
- Early mobilisation was achieved
- Aesthetic outcomes were satisfactory at 3-month follow-up
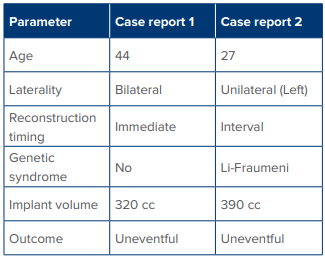
Table 1: Comparison of both reconstructive surgeries
Discussion
Implant-based breast reconstruction following NSM is increasingly recognised as a safe and effective approach in selected breast cancer patients. Preservation of the NAC significantly enhances aesthetic outcomes and patient satisfaction without compromising oncologic safety when appropriate criteria are met.2,3
Immediate reconstruction, as demonstrated in case report 1, offers several advantages, including reduced psychological distress, improved body image, and avoidance of additional surgeries. In contrast, interval reconstruction, as in case report 2, is particularly valuable in patients requiring prior oncologic treatment or in those with genetic syndromes such as Li-Fraumeni, where radiotherapy is contraindicated due to increased risk of secondary malignancies.6
The use of ADM in implant-based reconstruction has revolutionised surgical outcomes by providing inferolateral support, improving implant positioning, and reducing capsular contracture rates. Subpectoral implant placement remains a widely used technique, offering additional soft tissue coverage and reduced complication rates.5
Both cases in this series highlight the importance of meticulous surgical technique, including preservation of flap vascularity, careful patient selection, and multidisciplinary planning. The absence of complications in our patients aligns with reported literature demonstrating low complication rates in NSM with implant-based reconstruction.
Although limited by a small sample size, this case series demonstrates the feasibility of implant-based reconstruction across diverse clinical scenarios, including bilateral disease and hereditary cancer syndromes.
Perioperative Figures 1–8


Figure 1A and B: Preoperative markings for nipple-sparing mastectomy.

Figure 2: Intraoperative image showing mastectomy specimen.
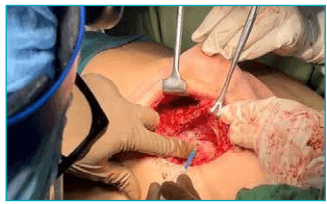
Figure 3: Creation of subpectoral pocket.
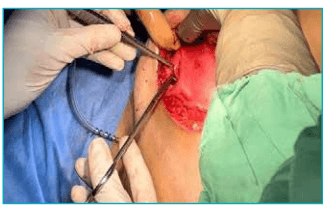
Figure 4: Acellular dermal matrix (ADM) placement and sling creation.

Figure 5: Implant positioning.

Figure 6: Immediate postoperative outcome.
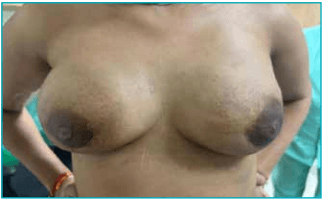
Figure 7: Bilateral reconstruction at 3 months follow-up.
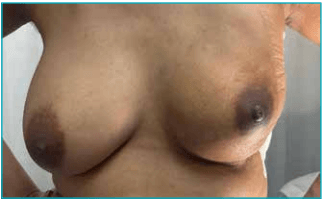
Figure 8: Unilateral reconstruction at 3 months follow-up.
Declarations
Ethics and consent
Written informed consent was obtained from both patients for publication. Institutional ethical guidelines were followed.
Artificial intelligence (AI) disclosure
The authors declare that artificial intelligence-assisted tools were used solely for language editing and manuscript structuring. All clinical content, data interpretation, and final manuscript approval were performed by the authors.
Conclusion:
Implant-based breast reconstruction following nipple-sparing mastectomy (NSM) is a safe, reproducible, and effective technique in both immediate and interval settings. Careful patient selection, adherence to oncologic principles, and multidisciplinary management are critical to achieving optimal outcomes. This approach provides excellent aesthetic results with minimal morbidity and high patient satisfaction.
Rajinder Kaur Saggu, Sneha Galande, Shreya Thakur, Riya Agrawal. Implant-Based Breast Reconstruction
Following Nipple-Sparing Mastectomy: A Case Series of Immediate and Interval Reconstruction in a
Dedicated Breast Unit. MMJ. 2026, March. Vol 3 (1).
References
- Cordeiro PG. Breast reconstruction after surgery for breast cancer. N Engl J Med. 2008;359(15):1590–601.
- Ananthakrishnan P, Feldman S. Nipple-sparing mastectomy: indications, oncologic safety. Minerva Chirurgica. 2012;67(3):257–70.
- De La Cruz L, Moody AM, Tappy EE, et al. Overall survival, disease-free survival, local recurrence, and nipple–areolar recurrence in the setting of nipple-sparing mastectomy: a meta-analysis and systematic review. Ann Surg Oncol. 2015; 22(10):3241–9.
- Albornoz CR, Bach PB, Mehrara BJ, et al. A paradigm shift in US breast reconstruction: increasing implant rates. Plast Reconstr Surg. 2013;131(1):15–23.
- Ibrahim AM, Koolen PG, Ashraf AA, et al. Acellular dermal matrix in reconstructive breast surgery: survey of current practice among plastic surgeons. Plast Reconstr Surg Glob Open. 2015;3(4):e381.
- Kratz CP, Achatz MI, Brugieres L, et al. Cancer screening recommendations for individuals with Li-Fraumeni syndrome. Clin Cancer Res. 2017;23(11):e38–45.