

Abstract:
Oocyte cryopreservation (OC), known as egg freezing, has transitioned from an experimental technique to an established component of modern reproductive medicine. Once limited by low survival rates, advances in laboratory cryobiology, particularly the vitrification process, have transformed this procedure as a viable option for fertility preservation across a wide range of clinical and social indications. This review traces the historical evolution of egg freezing, explains the biological and technical principles underlying the procedure and highlights its indications, risks, benefits, and limitations along with ethical viewpoints.
This review delineates various indications for fertility preservation, encompassing elective or social egg freezing for age-related fertility decline, non-malignant diseases such as endometriosis, autoimmune disorders, genetic predispositions to premature ovarian insufficiency, and oncofertility. Recent advancements, such as newer stimulation protocols including dual or double stimulation along with enhancements in vitrification techniques, are progressively refining clinical practice and outcomes. This article highlights the current evidence, clinical outcomes, and nuanced realities of egg freezing, emphasising the importance of informed decision-making and realistic expectations in reproductive planning.
Key words: Egg Freezing, Social Egg Freezing, Fertility Preservation, Oocyte Cryopreservation, Vitrification.
Introduction
Over the last two decades, reproductive timelines have shifted dramatically across societies. Women are pursuing higher education, professional careers, financial stability, and personal milestones before considering parenthood. Simultaneously, survival rates in cancer and other chronic illnesses have improved, bringing fertility preservation into sharp clinical focus. Against this backdrop, egg freezing has emerged as a powerful, yet often misunderstood tool.
Egg freezing resides at the intersection of medicine, ethics, economics, and societal transformation. The realities and nuances of egg freezing encompass the inherent biological limitations of reproductive ageing, inter-individual variability in ovarian response, laboratorydependent factors, and disparities in costs and access, with unpredictability in forecasting individual live birth outcomes.1 However, widespread awareness has also brought misconceptions such as “fertility insurance,” a phrase that oversimplifies biological reality and understates its inherent uncertainties.
For clinicians outside reproductive medicine, the challenge lies in understanding where egg freezing is genuinely beneficial, what its risks are, and how to counsel patients accurately. This review aims to bridge that gap by providing a practical, evidence-based framework to understand egg freezing in contemporary clinical practice.2,3
Methodology
This review was conducted as a narrative analysis based on a comprehensive literature search to consolidate existing knowledge on oocyte cryopreservation (OC), with a focus on its clinical implications and subtleties. A thorough search of PubMed/MEDLINE was performed to identify relevant peer-reviewed publications in English.
Eligible publications encompassed original research, systematic reviews, meta-analyses, narrative reviews and professional society guidelines addressing technical aspects, clinical outcomes, medical and nonmedical indications, effectiveness, safety, and ethical considerations of OC. Animal studies and single case reports were omitted. Data were qualitatively analysed and thematically categorised in accordance with the objectives of the review.
Historical Evolution of Egg Freezing
For several decades, egg freezing remained an experimental procedure dating back to the early 1980s. Early lab techniques like slow-freezing frequently resulted in ice crystal formation, meiotic spindle damage and chromosomal misalignment, leading to inconsistent survival and pregnancy rates.1
By the late 2000s, a major turning point occurred with the introduction of vitrification, a rapid freezing technique where the oocytes are cooled rapidly to -196 °C, and they become vitrified or “glass-like”. This significantly reduces the chances of ice crystal formation with improved oocyte survival, fertilisation, and embryo development rates. In 2012–2013, the American Society for Reproductive Medicine (ASRM) formally removed the “Experimental” label from egg freezing, recognising it as an established clinical procedure. This reclassification paved the way for broader applications, including elective (social) egg freezing and fertility preservation for medical indications.2,3
Biology of the Oocyte: Why Freezing Is Uniquely Challenging1,2
An understanding of oocyte biology is fundamental to appreciating the challenges of egg freezing. Human oocytes are the largest cells in the body, rich in cytoplasm and water content. They are arrested in metaphase II of meiosis, containing a delicate spindle apparatus essential for accurate chromosomal segregation.
Female reproductive ageing is characterised by both a quantitative and qualitative decline in oocytes. With advancing age, rates of aneuploidy increase, mitochondrial function deteriorates, and deoxyribonucleic acid (DNA) repair capacity diminishes.
Egg freezing does not reverse ageing; it merely pauses the biological clock at the age at which the eggs are frozen. This distinction is critical in patient counselling.
Indications of Egg Freezing4,5
I. Elective (Social) fertility preservation
Social egg freezing refers to fertility preservation undertaken without an immediate medical indication, allowing women to plan parenthood according to personal, professional and social considerations. Age at freezing remains the most important determinant of success. Optimal outcomes are observed when freezing is performed before 35 years of age, with diminishing benefits beyond 38 years and significantly reduced success after 40 years.6
II. Reproductive health concerns
Endometriosis
Endometriosis poses a unique challenge. Both the disease and its surgical treatment can compromise ovarian reserve. Egg freezing may be considered prior to ovarian endometrioma surgery or in women demonstrating declining ovarian reserve with endometriosis.
Genetic diseases
Primary ovarian insufficiency (POI), Turner syndrome, Fragile X premutation, X chromosome deletion, etc.
Autoimmune diseases
Conditions like systemic lupus erythematosus (SLE) may necessitate gonadotoxic therapies, warranting fertility preservation.
III. Oncofertility
Fertility preservation is now an integral component of cancer care. Egg freezing is recommended for women undergoing various oncological treatments such as chemotherapy, radiation, bone marrow transplantation amongst others.
IV. Male factor
Surgical sperm retrieval surgery: Where sperm retrieval is unsuccessful, no sperm are retrieved on the day of oocyte retrieval, or the husband's unavailability on the day of oocyte retrieval.
V. Donor oocyte banking/Assisted reproductive technology (ART) banks
Enhances flexibility and availability in egg donation cycles, allowing better synchronisation and wider access.
VI. Fertility preservation in transgender men
Prior to gender-affirming treatment.
Step-by-Step Egg Freezing Procedure2,4,5
I. Patient selection, counselling and screening
The process begins with a comprehensive evaluation involving consultations with a fertility specialist and tests to assess ovarian reserve and overall health. Counselling must emphasise that outcomes are probabilistic rather than guaranteed.
Key considerations include:
- Chronological age
- Ovarian reserve markers (reproductive hormone blood tests like follicle-stimulating hormone [FSH], luteinising hormone [LH], oestradiol, and anti-Müllerian hormone (AMH); ultrasound parameter: antral follicle count)
- Medical history (endometriosis, tuberculosis, autoimmune disorders, prior ovarian surgery, cancer and onco-therapies)
- Reproductive goals and timelines
II. Controlled ovarian stimulation and egg retrieval procedure
Controlled ovarian stimulation involves daily hormonal injections to induce multifollicular development, monitored through ultrasounds and hormonal assays to tailor the individual response. Once the follicles attain the desired size, transvaginal ultrasoundguided oocyte retrieval is performed under short general anaesthesia as a day care procedure. The procedure is generally safe, with low complication rates. Typically, this process starts during the first 2–3 days of menstruation. It requires approximately 2–3 weeks for completion. However, in oncology patients, it is initiated anytime during the menstrual cycle as a random-start stimulation protocol.
III. Laboratory aspects of oocyte freezing: Vitrification
Retrieved oocytes are assessed by an embryologist and the mature metaphase II oocytes are cryopreserved using the vitrification process (Figure 1). Vitrification is now the global gold standard, achieving post-thaw survival rates exceeding 90%, with fertilisation and implantation rates comparable to fresh oocytes.7
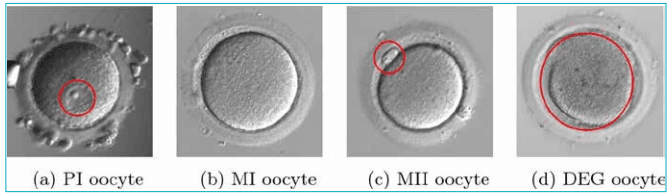
Figure 1: Stages of oocyte maturation: A. Prophase I – Geminal vesicle; B. Metaphase I oocyte; C. Metaphase II oocyte with polar body; D. Degenerated oocyte.8
Abbreviations: DEG: Degenerated Oocyte; MI: Metaphase I; MII: Metaphase II; PI: Prophase I.
Risks and complications9
A. Short-term risks: Ovarian hyperstimulation syndrome (OHSS), procedural complications related to oocyte retrieval and anaesthetic risks
B. Emotional and financial burden: Distress if expectations are unrealistic, or if multiple cycles are required
C. False reassurance: No oocytes retrieved, empty follicle syndrome, or no mature metaphase II (MII)oocytes suitable for freezing
D. Long-term risks: Maternal and paternal age at pregnancy: Obstetric risks like miscarriages,congenital anomalies, gestational diabetes mellitus, pre-eclampsia, preterm labour, foetal growth restriction
Optimal Age and success rate
Egg quality declines non-linearly, accelerating after 35 years of age. The probability of a live birth derived from preserved oocytes is around 60% in women younger than 35 years and 29% in women older than 35 years. Considering cumulative attrition across all stages, cryopreservation of approximately 8–15 mature oocytes in women younger than 35 years and 15–20 oocytes in women older than 35 years is recommended to achieve a projected 60%–70% chance of live birth.6 Notably, a 42-year-old woman has a 6.6% chance of giving birth with her own fresh oocytes, whereas if she freezes her eggs at the age of 30, she has more than 40% chance of a successful live birth.10 These findings highlight that freezing fewer, better quality eggs under 35 years yields optimal outcomes (Table 1).
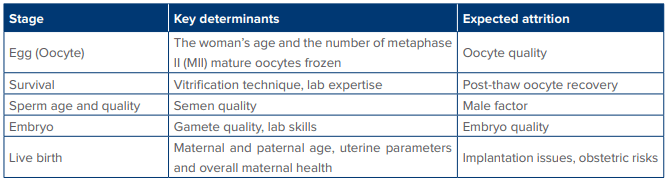
Table 1: Determinants of success.
Myths, nuances, and reality
- Myth: Egg freezing guarantees future pregnancy; Reality: Egg freezing preserves potential but does not guarantee a live birth.
- Myth:Age alone matters; Reality: The number of oocytes frozen matters as much due to attrition effects and is age-stratified.
- Myth:Hormone stimulation leads to long-term endocrine or oncological risks; Reality: Current evidence shows that ovarian stimulation produces short-term hormone exposure and is not associated with a demonstrable increase in cancer risks.
- Myth:Egg Freezing is better than embryo freezing; Reality: Embryo freezing has a higher per-unit successful live birth rate.
- Myth:Vitrification is a perfect ‘time capsule’; Reality: It is not a rejuvenation machine that stops ageing or repairs DNA damage.
Changing Trends and Usage Rates of Frozen Oocytes
A retrospective 12-year study conducted by Rohatgi et al. and presented at the Royal College of Obstetricians and Gynaecologists (RCOG) World Congress, London, 2025, highlighted a favourable transition in reproductive dynamics in urban India, with egg freezing gaining recognition as a reproductive choice that enhances individual reproductive autonomy. Interestingly, following the coronavirus disease 2019 (COVID-19) pandemic, there was a sharp rise (67.25%) in the number of women who underwent social egg freezing, in contrast to only 24.6% pre-COVID-19. The most common age group was 31–35 years (37.70%), followed by 36-40 years (32.8 %) and the oldest was 47 years of age. Total 9.83% had repeat egg freezing cycles, and again maximum repeat cycles were done post pandemic in the year 2023 in the age group of 35–36 years. Another interesting finding of this study was a low utilisation rate of only 9.8%, underscoring societal challenges and financial limitations. These findings emphasise the need for strengthened education and support to empower women in planning their reproductive journeys.
Egg Freezing in India: Legal and Ethical Considerations
In India, egg freezing is regulated under the Assisted Reproductive Technology (Regulation) Act, 2021 and corresponding rules. It occupies a distinctive legal and ethical position within assisted reproduction involving invasive medical intervention for future therapeutic intent, thus creating long-lived reproductive material for deferred use and sits at the intersection of autonomy, futureoriented consent, equity and responsibility with emerging challenges posed by extended storage, posthumous use and evolving technologies.11
Technological Advances in Egg Freezing12
- Vitrification 2.0 and automated freezing systems reduce manual error and improve post-thaw survival rates.
- Artificial intelligence (AI) in OC involves non-invasive analysis tools such as VIOLET, which uses a light microscope to capture images of mature oocytes before freezing and instantly grades the quality of each egg, giving more individualised data for blastocyst formation and its potential live birth outcomes.
- AI-driven timing optimisation using the IndividuaLised oocyte retrieval Estimator based on gradient-boosted Trees Integrating Attentions (IL-ETIA) forecasts the optimal interval between ovulation trigger and oocyte retrieval.
- AI-guided mechanical oocyte profiling utilises a novel instrument with micromachined probes to measure an egg’s mechanical properties non-destructively, giving a quantitative quality score prior to freezing.
- Artificial ovary constructs are scaffolds seeded with follicles designed to mimic natural ovarian function.
- In vitro maturation (IVM) refers to the maturation of immature oocytes in vitro in the laboratory.
Conclusion:
Egg freezing, as a reproductive choice, sits at the intersection of biology, probability, technology and social narrative. It is a powerful tool when paired with timely planning, judicious counselling, and realistic expectations. Today, egg freezing in India is emerging as a strategic technological advancement, translating OC from promise to practice.
Tanya Buckshee Rohatgi, Nipasa Sarma. Egg Freezing: From Experimental Concept to Mainstream
Reproductive Strategy — Process, Nuances, and Clinical Reality. MMJ. 2026, March. Vol 3 (1).
References
- Hirsch A, Hirsh Raccah B, Rotem R, et al. Planned oocyte cryopreservation: a systematic review and meta-regression analysis. Hum Reprod Update. 2024;30(5):558–68.
- Practice Committees of the American Society for Reproductive Medicine and the Society for Assisted Reproductive Technology. Mature oocyte cryopreservation: a guideline. Fertil Steril. 2013;99(1):37–43.
- Ethics Committee of the American Society for Reproductive Medicine. Planned oocyte cryopreservation to preserve future reproductive potential: an Ethics Committee opinion. Fertil Steril. 2024;121(4):604–12.
- Oktay K, Harvey BE, Partridge AH, et al. Fertility preservation in patients with cancer: ASCO clinical practice guideline update. J Clin Oncol. 2018;36(19):1994–2001.
- Cobo A, Diaz C. Clinical application of oocyte vitrification: a systematic review and meta-analysis of randomized controlled trials. Fertil Steril. 2011;96(2):277–85.
- Mertes H, Pennings G. Social egg freezing: for better, not for worse. Reprod Biomed Online. 2011;23(7):824–9.
- Papatheodorou A, Vanderzwalmen P, Panagiotidis Y, et al. Open versus closed oocyte vitrification system: a prospective randomized sibling-oocyte study. Reprod Biomed Online. 2013;26(6):595–602.
- Targosz A, Myszor D, Mrugacz G. Human oocytes image classification method based on deep neural networks. Biomed Eng Online. 2023;22(1):92.
- Pantos K, Maziotis E, Trypidi A, et al. The effect of open and closed oocyte vitrification systems on embryo development: a systematic review and network meta-analysis. J Clin Med. 2024;13(9):2651.
- Chronopoulou E, Raperport C, Sfakianakis A, et al. Elective oocyte cryopreservation for age-related fertility decline. J Assist Reprod Genet. 2021;38(5):1177–86.
- Government of India. The Assisted Reproductive Technology (Regulation) Act, 2021. No. 42 of 2021. Gazette of India; 2021. Available at: https://www.indiacode.nic.in/ bitstream/123456789/17031/1/aA2021-42.pdf. Accessed on: 20th December 2025.
- Peschansky C, Patel S, Amir J, et al. Picture perfect?: determining the clinical utilization of artificial intelligence in oocyte cryopreservation. Fertil Steril. 2021;116(3 Suppl):e157.