

Abstract:
When we meet any individual, the first feature we tend to notice is their smile. An aesthetically pleasing smile plays a pivotal role in a person’s self-esteem and confidence. We can state that when an aesthetic dentist performs smile makeover procedures, they aim to improve dental aesthetics and patient confidence. There are many techniques to perform a smile makeover, from composite bonding, orthodontic treatments, dental implants and ceramic restorations. This article explains the steps involved in a smile makeover with ceramic restoration, including veneers, crowns and partial crowns. It also explains which individuals can opt for a smile makeover procedure, along with multiple case presentations. A smile makeover with ceramic restoration is an efficient treatment option to improve the shape, shade, alignment and orientation of an individual’s teeth in a relatively short time span.
Key words: Ceramic/e.max Veneers and Crowns, 3D Smile Design, Smile Makeover, Orthodontics,Composite Bonding.
Introduction
What does a smile makeover mean?
A smile makeover can be defined as a procedure that enables the transformation of an imperfect and unattractive smile into a beautiful, aesthetically pleasing smile by means of various dental interventions.1–3 These procedures could include the use of composite or ceramic veneers, metal-free crowns, dental implants, teeth whitening, gum contouring and orthodontics.
Who could need a smile makeover?
A smile makeover may be indicated for individuals who are dissatisfied with the appearance of their smile and seek improvement in dental aesthetics and function. Patients commonly present with concerns such as tooth discolouration, enamel wear, chipped or fractured teeth, spacing between teeth, mild-to-moderate malalignment, protrusion, or missing teeth. Additionally, uneven gingival architecture, gingival pigmentation, and teeth that are disproportionate to facial features may adversely affect smile harmony and warrant aesthetic intervention. Smile makeover procedures are also beneficial for patients with altered tooth form or orientation due to parafunctional habits, erosion, or previous dental treatments. Appropriate case selection, based on clinical examination, patient expectations, and periodontal and occlusal health, is essential to determine the most suitable treatment approach and to achieve predictable and satisfactory outcomes.1,2,4
What are the procedures involved for a smile makeover?
The procedures involved in a smile makeover include orthodontic treatment for the correction of tooth alignment, teeth whitening to improve dental shade, and dental implants for the replacement of missing teeth. Composite bonding may be used for minor aesthetic corrections, such as closing small spaces or repairing chipped teeth, while periodontal procedures, such as gum contouring or depigmentation, help enhance gingival symmetry and appearance. Fixed prosthetic options, including crowns and bridges, are employed to restore tooth form, function, and aesthetics, whereas ceramic veneers are commonly used to modify tooth colour, shape, size, and alignment to achieve an overall harmonious smile.5–7 In this article, we will be emphasising on ceramic veneers. Ceramic veneers are thin layers of porcelain cemented onto the outer surface of the tooth enamel to achieve the desired aesthetic and functional result (Figure 1). This may involve minimal preparation or trimming of the tooth enamel.1,4,6 These shells are bonded to the front of the teeth, thereby changing their colour, shape, size, or length.

Figure 1:Representative clinical image illustrating a ceramic veneer bonded to the labial surface of anterior teeth to enhance aesthetics.
Why ceramic veneers?
The advantages and limitations of orthodontic treatment,composite bonding, and ceramic veneers are summarised in Table 1.1,6,7
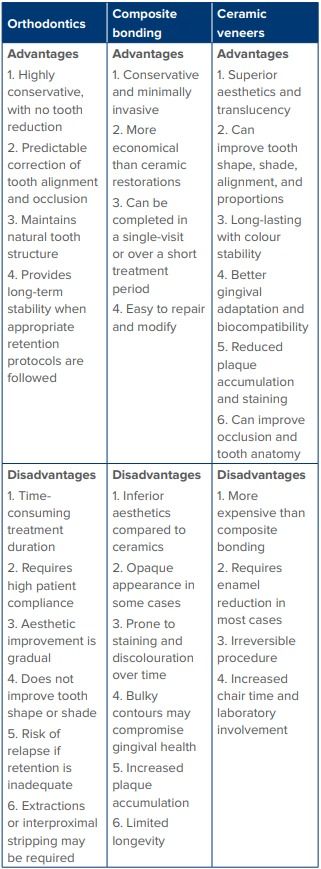
Table 1: Advantages and limitations of orthodontic treatment,composite bonding, and ceramic veneers.
Steps for Smile Makeover
- Pictures, videos, and impressions or scans
- Three-dimensional (3D) smile design
- Mock-up
- Teeth preparation or veneer preparation
- Temporisation or trial smile
- Review to check the trial smile and make changes in the temporaries, if needed
- Trials and cementation
- Follow-up
Where do we start?
Smile makeover treatment begins with comprehensive data collection to accurately assess the patient’s existing dental and facial parameters before formulating a definitive treatment plan. Diagnostic records include intraoral impressions using elastomeric materials or digital intraoral scans to document the patient’s pretreatment dental condition and occlusion (Figure 2). Standardised extraoral and intraoral photographs and videos are recorded8,9 using a digital single-lens reflex (DSLR) camera to evaluate smile dynamics, tooth display, facial symmetry, and lip mobility, and to facilitate effective communication between the clinician and the laboratory technician (Figure 3, Figure 4A and B). When indicated, a face-bow transfer is performed to record the maxillomandibular relationship and to accurately transfer functional and aesthetic parameters to the articulator for precise treatment planning (Figure 5). In addition to clinical records, understanding patient expectations is a critical component of smile design, as it helps align the proposed aesthetic outcome with the patient’s concerns and desired improvements, thereby enhancing acceptance and predictability of the final result.
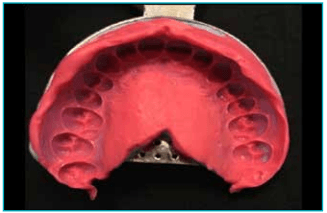
Figure 2: Intraoral impressions or digital scans recorded as part of pre-treatment diagnostic data collection.

Figure 3: Digital single-lens reflex (DSLR) camera for pretreatment smile analysis and documentation.
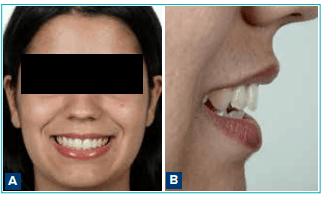
Figure 4A and B: Standardised frontal and lateral extraoral facial photographs used for smile analysis and digital smile design.
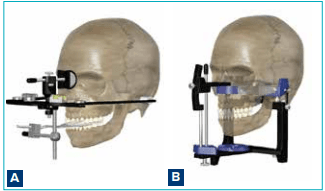
Figure 5A and B: Face-bow transfer procedure used to record maxillomandibular relationships and to transfer them accurately to the articulator.
3D smile design
This is a technique used to envision the final result before beginning the case. By utilising the patient’s pictures, impressions, or scans, a digital smile design software like Digital Smile Design (DSD) and Exocad Dental Computer-Aided Design (CAD) is used to create the design of an individual’s future smile on a 3D model with facial simulation. This helps the patient understand and accept the treatment plan better.8,9
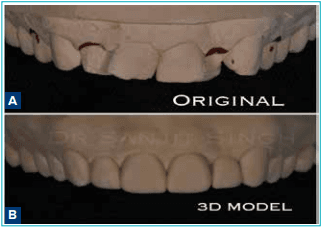
Figure 6A and B: Digital smile design workflow demonstrating the integration of patient photographs and dental scans for virtual smile planning.

Figure 7A and B: Three-dimensional (3D) digital smile design model illustrating proposed teeth dimensions, contours, and smile harmony.
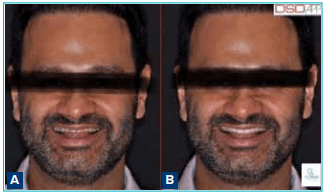
Figure 8A and B: Facial simulation depicting pre-treatment and post-treatment smile outcomes using digital smile design software.
Mock-up
This is a technique used to transfer the new 3D smile onto the patient’s existing teeth without altering the patient’s original teeth. This mock-up acts as a test drive for the patient, allowing them to see what their future smile would look like even before any tooth preparation begins.4
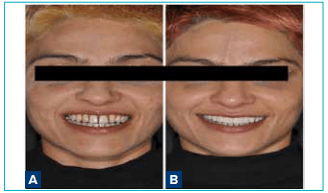
Figure 9A and B: Intraoral mock-up transferred from the digital smile design to the patient’s existing dentition without tooth preparation.
Tooth preparation
After the patient is anaesthetised, selective trimming of tooth enamel is performed to make space for the ceramic e.max veneer. The amount of tooth preparation needed is guided by the 3D smile design model.1,7 Incisal and labial guides are fabricated from the 3D model.
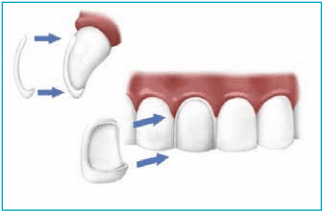
Figure 10: Tooth preparation design for ceramic veneers demonstrating minimal reduction confined to the labial surface with an incisal butt-joint configuration.

Figure 11: Pre-operative view of anterior teeth before veneer tooth preparation.

Figure 12: Post-preparation view showing minimal enamel reduction following guided veneer preparation.
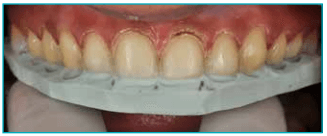
Figure 13: Incisal reduction guide (incisal index) used to verify adequate and controlled tooth preparation.
Temporisation
Once tooth preparation is complete, the patient is fitted with temporary veneers or restorations crafted intraorally from a putty index derived from the 3D smile design model. These temporaries utilise bis-acryl composite materials, such as Protemp or Luxatemp, ensuring optimal fit, aesthetics, and comfort during the interim period.

Figure 14: Putty index derived from the digital smile design used for the fabrication of provisional restorations.
Veneer cementation
The dental laboratory typically requires about one week to fabricate the final veneers,6,7 most commonly using e.max lithium disilicate or feldspathic porcelain for their strength, aesthetics, and biocompatibility.
Prior to cementation, a trial fitting is performed to confirm the fit, shape, and shade with the patient. Upon approval, the veneers are bonded using a meticulous protocol tailored to the material, ensuring long-term durability and natural results.

Figure 15A and B: Comparison of anterior teeth before and after cementation of lithium disilicate (e.max) ceramic veneers.
Follow-up
A follow-up appointment is scheduled a few days postcementation to verify optimal bite, occlusion, and overall comfort. This step ensures that any minor adjustments are addressed promptly, maximising patient satisfaction and the longevity of the veneers.
Clinical Cases
To illustrate the transformative results of our protocol, we present selected clinical cases below. These feature before-and-after comparisons of patients who received ceramic restorations and veneers,10 highlighting enhanced aesthetics, function, and patient satisfaction.
Case report 1
A female patient in her mid-30s presented with severe erosion and tooth wear caused by long-standing gastric reflux and bruxism. Loss of anterior tooth length not only compromises masticatory efficiency but also contributes to a prematurely aged appearance. The patient’s primary objective was to restore a youthful smile using ceramic restorations. As the patient was travelling from London specifically for dental treatment, comprehensive digital planning was performed in advance, including a 3D smile design prior to her arrival in India. The treatment was completed within 10 days using lithium disilicate (e.max) veneers and partial crowns, achieving both functional and aesthetic rehabilitation.
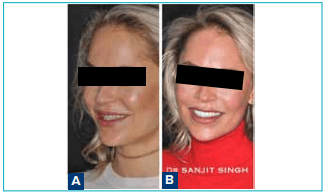
Figure 16: A. Pre-treatment extraoral and intraoral views showing severe erosion and wear of the anterior teeth due to gastric reflux and bruxism; B. Post-treatment views demonstrating restoration of tooth length and smile aesthetics using ceramic restorations.

Figure 17: A. Pre-treatment smile view illustrating reduced incisal display and an aged appearance; B. Post-treatment smile view showing improved incisal display, tooth proportions, and overall facial harmony.
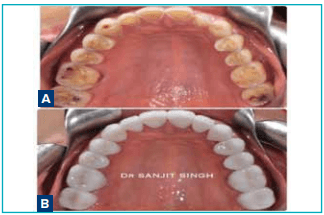
Figure 18 A and B: Comparison of anterior teeth before and after cementation of lithium disilicate (e.max) ceramic veneers.
Case report 2
A female patient in her mid-30s presented with severe erosion and tooth wear caused by long-standing gastric reflux and bruxism. Loss of anterior tooth length not only compromises masticatory efficiency but also contributes to a prematurely aged appearance. The patient’s primary objective was to restore a youthful smile using ceramic restorations. As the patient was travelling from London specifically for dental treatment, comprehensive digital planning was performed in advance, including a 3D smile design prior to her arrival in India. The treatment was completed within 10 days using lithium disilicate (e.max) veneers and partial crowns, achieving both functional and aesthetic rehabilitation.

Figure 19 : A. Pre-treatment extraoral and intraoral views showing anterior spacing, protrusion, and excessive gingival display;B. Post-treatment views demonstrating space closure, reduced gingival display, and improved smile aesthetics.

Figure 20 : A. Pre-treatment digital smile analysis;B.Post-treatment digital smile design illustrating proposed tooth proportions and gingival correction.

Figure 21 : A. Pre-treatment intraoral view prior to veneer preparation; B. Post-preparation view following guided minimal tooth reduction
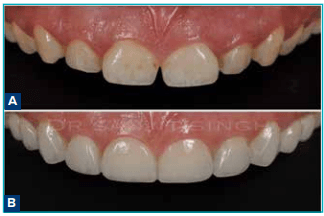
Figure 22 : A. Pre-treatment smile view showing spacing and shade discrepancies; B. Post-treatment smile view demonstrating improved tooth shade, form, and harmonious smile design.
Case report 3
This case involved a patient residing in the United States who presented with crowded and discoloured anterior teeth. Ideally, such cases are best managed with orthodontic treatment. However, due to the patient’s psychological distress, including depression and lack of self-confidence, a restorative approach was selected at the insistence of his family. In cases requiring significant alteration of tooth position and appearance, a 3D smile design is essential to accurately visualise the final outcome prior to initiating treatment. After achieving a satisfactory digital simulation, the treatment plan was approved. Although increased tooth preparation was anticipated and posed a concern, careful planning allowed completion of treatment without the need for endodontic intervention, resulting in a successful aesthetic outcome.
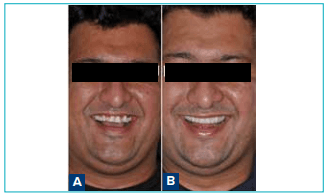
Figure 23 : A. Pre-treatment intraoral views showing crowded and discoloured anterior teeth; B. Post-treatment views demonstrating correction of crowding and improved tooth shade with ceramic restorations.
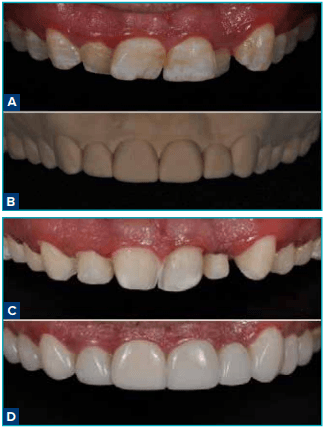
Figure 24 : Sequential views illustrating: A. Pre-treatment condition; B. Digital smile design; C. Tooth preparation; D. Final restorative outcome.
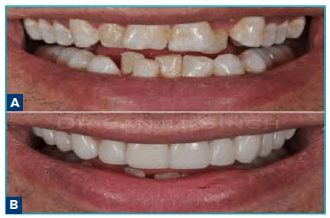
Figure 25 : A. Pre-treatment frontal smile view showing irregular alignment; B. Post-treatment frontal smile view demonstrating improved smile symmetry.

Figure 26 : A. Pre-treatment lateral smile view; B. Post-treatment lateral smile view showing improved facial harmony.

Figure 27 : A. Pre-treatment intraoral frontal view showing crowding and discolouration;B. Post-treatment intraoral frontal view demonstrating improved alignment, shade, and symmetry following ceramic restorations.
Case report 4
This patient had previously undergone orthodontic treatment; however, residual spacing remained, resulting in compromised smile aesthetics. A restorative approach using ceramic veneers and partial restorations was employed to correct the spacing and enhance overall dental harmony. The case was managed using an interdisciplinary approach involving a periodontist and an orthodontist to ensure optimal aesthetics, function, and long-term stability.

Figure 28 : A. Pre-treatment intraoral view showing residual spacing following orthodontic treatment; B. Post-treatment views after correction with ceramic veneers and partial restorations.

Figure 29 : A. Pre-treatment smile view with residual spacing and compromised aesthetics;B. Post-treatment smile view demonstrating improved dental harmony and proportions.
Case report 5
This case involved a young patient who had lost her maxillary anterior teeth and required placement of two dental implants along with guided bone regeneration. Additional procedures included gingival crown lengthening performed using a diode laser to achieve optimal soft-tissue aesthetics. A multidisciplinary treatment approach was adopted to create a harmonious and natural-looking smile. The total treatment duration was approximately one year, allowing sufficient time for implant osseointegration prior to veneer placement. Final rehabilitation included a combination of implantsupported crowns, endodontic treatment, and lithium disilicate (e.max) veneers.

Figure 30 : A. Pre-treatment views showing missing maxillary anterior teeth; B. Post-treatment view demonstrating restored smile aesthetics following multidisciplinary rehabilitation.
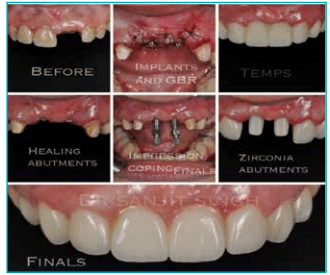
Figure 31 : Sequential images showing implant placement and guided bone regeneration in the maxillary anterior region.
Abbreviation: GBR: Guided Bone Regeneration.
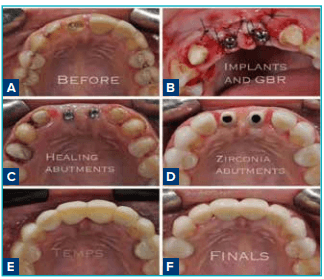
Figure 32 : A. Pre-treatment soft-tissue condition;B-F. Healing,provisionalisation, and soft-tissue contouring prior to final restoration.
Abbreviation: GBR: Guided Bone Regeneration.
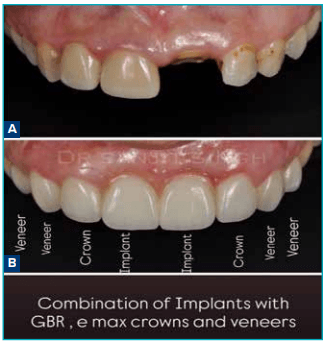
Figure 33 : A. Pre-treatment smile view with missing anterior teeth;B. Post-treatment smile view showing implant-supported restorations combined with ceramic veneers and crowns.
Abbreviation: GBR: Guided Bone Regeneration.
Case report 6
This patient presented with discoloured teeth caused by dental fluorosis, characterised by dark, patchy enamel discolouration that negatively impacted her self-esteem. The patient desired a brighter and more uniform smile. Ceramic lithium disilicate (e.max) veneers were used to mask the discolouration effectively and restore an aesthetically pleasing smile.
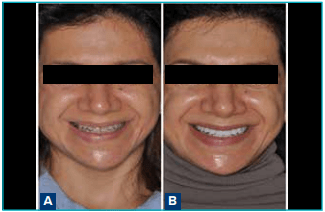
Figure 34 : A. Pre-treatment intraoral views showing enamel discolouration due to fluorosis; B. Post-treatment views demonstrating masking of discolouration with ceramic veneers.

Figure 35 : A. Pre-treatment smile view with uneven tooth shade; B. Post-treatment smile view showing a brighter and more uniform smile.
Case report 7
This case involved a patient who presented with an anterior diastema and dissatisfaction with tooth shade and shape. A restorative treatment plan using ceramic veneers and partial crowns was implemented to close the spaces and improve tooth proportions, resulting in a balanced and aesthetically pleasing smile.
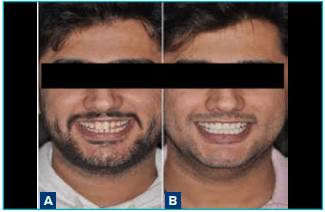
Figure 36 : A. Pre-treatment intraoral views showing anterior diastema; B. Post-treatment view demonstrating diastema closure with ceramic restorations.

Figure 37 : A. Pre-treatment smile view with spacing and shape discrepancies; B. Post-treatment smile view showing improved aesthetics with ceramic veneers and partial crowns.
Case report 8
This patient presented with multiple carious lesions accompanied by pain and significant concern regarding her smile appearance. Initial management included comprehensive caries removal, composite restorations, and necessary endodontic treatment. Subsequently, a combination of lithium disilicate (e.max) veneers and crowns was used to achieve functional rehabilitation and a complete aesthetic transformation.
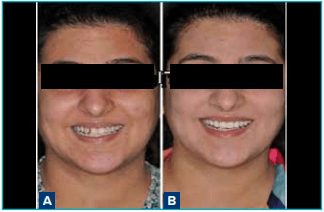
Figure 38 : A. Pre-treatment intraoral views showing multiple carious lesions; B. Post-treatment views following caries management and aesthetic rehabilitation.

Figure 39 : A. Pre-treatment view prior to definitive restorations; B. Post-treatment view after placement of ceramic veneers and crowns.

Figure 40 : A. Pre-treatment smile view with compromised aesthetics; B. Post-treatment smile view demonstrating complete functional and aesthetic rehabilitation.
Conclusion:
Smile makeovers using ceramic veneers and partial crowns provide a predictable and efficient solution for improving dental aesthetics and function in appropriately selected patients. With careful diagnosis, structured treatment planning, and the use of digital tools such as 3D smile design, clinicians can accurately visualise outcomes, enhance patient communication, and achieve high levels of satisfaction.
Ceramic restorations offer excellent aesthetics, durability, and favourable gingival response, making them a reliable alternative to orthodontic treatment in patients seeking immediate aesthetic improvement. When performed by a trained aesthetic dentist, smile makeover procedures not only enhance dental appearance but also significantly improve patient confidence and overall quality of life.
Sanjit Singh. Smile Makeover with Ceramic Restorations Without Orthodontic Intervention: A Case
Series. MMJ. 2026, March. Vol 3 (1).
March. Vol 3 (1).
References
- 1.Minase DA, Sathe S, Bhoyar A, et al. Porcelain Laminate Veneers: A Case Report. Cureus. 2023;15(1):e34220.
- Fradeani M, Barducci G. Esthetic rehabilitation in fixed prosthodontics. Quintessence Publishing Company; 2008.
- Korkut B. Smile makeover with direct composite veneers: A two-year follow-up report. J Dent Res Dent Clin Dent Prospects.2018;12(2):146.
- Gurel G, Morimoto S, Calamita MA, et al. Clinical performance of porcelain laminate veneers: outcomes of the aesthetic pre-evaluative temporary (APT) technique. Int J Periodontics Restorative Dent. 2012;32(6).
- Magne P, Belser UC. Porcelain versus composite inlays/ onlays: effects of mechanical loads on stress distribution, adhesion, and crown flexure. Int J Periodontics Restorative Dent. 2003;23(6):543–55.
- Guess PC, Stappert CF. Midterm results of a 5-year prospective clinical investigation of extended ceramic veneers. Dent Mater.2008;24(6):804–13.
- Stappert CF, Ozden U, Gerds T, et al. Longevity and failure load of ceramic veneers with different preparation designs after exposure to masticatory simulation. J Prosthet Dent.2005;94(2):132–9.
- Thomas PA, Krishnamoorthi D, Mohan J, et al. Digital Smile Design. J Pharm Bioallied Sci. 2022;14(Suppl 1):S43–9.
- Coachman C, Paravina RD. Digitally Enhanced Esthetic Dentistry- From Treatment Planning to Quality Control. J Esthet Restor Dent. 2016;28 Suppl 1:S3–4.
- Oquendo A, Brea L, David S. Diastema: correction of excessive spaces in the esthetic zone. Dent Clin North Am.2011;55(2):265–81, viii.