

Abstract:
Breasts can be the target organ for many autoimmune conditions. Pregnancy is a known trigger for flares of autoimmunity. Sometimes, inflammation limited to the breast is the first symptom of a systemic autoimmune disease. However, due to the rarity of this presentation, the diagnosis of a pregnancy-induced autoimmune breast inflammation can be very difficult. A young woman presented in the 12th week of her pregnancy with persistent symptoms of pain and erythema of the breast. She underwent repeated imaging investigations and received multiple courses of antibiotics without relief. Within a few weeks, she also developed massive enlargement of her breasts. Even though she was evaluated for a possible autoimmune aetiology, the test results could not clinch a diagnosis. In view of the development of gigantomastia by the third trimester, delivery was induced at 30 weeks. Lactation was suppressed with cabergoline. Two weeks after delivery, she started manifesting symptoms of systemic autoimmune disease, and after detailed evaluation, was diagnosed with systemic lupus erythematosus with Sjögren’s syndrome. After appropriate medication, her disease went into remission, and the gigantomastia regressed to near-normal size. A diagnosis of autoimmune mastitis should be kept in mind in patients with persistent inflammation of the breast. An early diagnosis may help detect systemic diseases and initiate a prompt, appropriate therapeutic strategy.
Key words: Autoimmune Mastitis, Gigantomastia Gravidorum, Systemic Lupus Erythematosus, Dopamine Agonists, Reduction Mammoplasty, Case Report.
Introduction
Inflammation of the breast due to infection is a common occurrence. Inflammatory carcinoma of the breast is the next most important diagnosis. Autoimmune mastitis belongs to a third group of aetiology.1 It includes conditions that are limited to the breast only, such as idiopathic granulomatous mastitis. It may also be part of the presentation of a wide range of autoimmune diseases, such as diabetes, thyroiditis, systemic erythematosus lupus (SLE), Sjögren’s syndrome, giant cell arteritis, polyarteritis nodosa, Behçet’s disease, sarcoidosis, Crohn’s disease, etc.2,3 However, breast-limited inflammation is sometimes the first symptom of a systemic autoimmune disease. The clinical picture of autoimmune mastitis may vary from being asymptomatic to presenting with severe, recurrent breast inflammation, painful nodules, nipple discharge or retraction, and lymphadenopathy. Gigantomastia gravidorum (GG) is another rare diagnosis, with a reported incidence of 1:28,000 to 1:100,000 pregnancies.4 It is characterised by rapid, diffuse, and excessive hypertrophy of the breasts, which requires reduction of more than 1500 g of tissue from each breast for relief of symptoms. 5 It is usually bilateral, presents during the 1st and early 2nd trimesters of pregnancy, and can give rise to a myriad of physical symptoms, such as breast pain, infection, ulceration, postural problems, back pain, and loss of nipple sensation.6 The aetiopathogenesis of gigantomastia is still not clearly understood. Theories such as end-organ hypersensitivity, hyperprolactinaemia, impaired liver function or steroid metabolism, autoimmune stimulation antibodies, and high insulin-like growth factor 1 (IGF-1) have been proposed.3,4 GG has been reported to be associated with various autoimmune disorders, such as SLE, myasthenia gravis, Graves’ disease, chronic arthritis, psoriasis, and Hashimoto’s thyroiditis.7,8 In a review of 108 patients with gigantomastia, 9.2% cases had autoimmune conditions.6 We present the case of a young woman who developed autoimmune mastitis with GG during her 4th pregnancy, and progressed to full-blown manifestation of SLE with Sjögren’s disease in the postpartum period, and discuss the challenges faced in managing this very rare clinical problem.
Case Report
A 28-year-old multigravida (gravida 4, para 1 plus 2 abortions [G4P1+2]) presented at 12 weeks of gestation in her 4th pregnancy with pain and redness of the skin over her left breast. There was no history of fever, prior illness, or medication use. However, her obstetric history was significant. She had to terminate her first pregnancy due to the absence of foetal cardiac activity. For her second pregnancy, she underwent a caesarean section in view of decreased foetal movements due to oligohydramnios. In the postpartum period, she developed a left breast abscess for which incision and drainage (I&D) was done. The third pregnancy was terminated, as it was unplanned. Her examination showed enlargement of both breasts with an area of erythema and tenderness in the left breast (Figure 1A and B). Skin oedema was present, with no palpable lump or fluctuation. Bilateral enlarged axillary accessory breasts were noted, along with a scar of I&D on the left breast. With a provisional diagnosis of mastitis, she was advised a course of antibiotics (Tab Augmentin 625 mg x thrice a day) for 7 days, without symptomatic relief. She continued to present for followup for over a month, with persistent symptoms and no abscess formation. Laboratory investigations were all within normal limits, and serial ultrasounds showed diffuse enlargement of both breasts without any focal lesion. Given concern for inflammatory carcinoma of the breast, a breast biopsy was performed, which showed mild chronic perivascular inflammation in the dermis, with no evidence of malignancy or granulomas. By the end of 20–22 weeks, she had developed gross enlargement of both breasts. Assessment of hormonal profile was done, and serum prolactin (186 ng/mL, range 10 to 209 ng/mL), thyroidstimulating hormone (TSH), follicle-stimulating hormone (FSH), luteinising hormone, and oestradiol were all found to be within normal limits. She was advised to take tablet cabergoline 0.5 mg twice weekly for about a month; however, breast enlargement continued, and skin showed patchy redness and peau d’orange appearance. With a possible diagnosis of autoimmune mastitis, she was further investigated. Inflammatory markers were raised (erythrocyte sedimentation rate [ESR] 58 mm/h; C-reactive protein [CRP] 9.34 mg/dL (normal < 0.6 mg/dL)]. Blood counts showed dimorphic anaemia (normocytic normochromic and microcytic hypochromic with mild anisocytosis), normal white blood cell (WBC) and platelet count. However, tests for autoantibodies (antinuclear antibody [ANA], rheumatoid factor [RF], and direct and indirect Coombs’ test) were all negative.

Figure 1A and B: Clinical presentation at 12 weeks of gestation showing pain and erythema of the left breast.
By 28 weeks of pregnancy, the breasts extended to the umbilicus in the sitting position, causing significant physical discomfort due to the excessive weight, without ulceration or necrosis of the skin (Figure 2A and B). With a diagnosis of GG, the patient was referred to a gynaecologist. After assessment of foetal maturity, a lower-segment caesarean section [LSCS] was performed at 30 weeks of gestation, delivering a healthy baby weighing 1.8 kg. Her lactation was suppressed by cabergoline.

Figure 2A and B: A. Gigantomastia gravidorum at 24 weeks of gestation; B. Progressive gigantomastia at 30 weeks of gestation. At 1 month postpartum, there was some reduction in breast size. However, she developed symptoms of joint pains and stiffness, and red scaly rashes on her face. She also complained of photosensitivity and redness of the eyes. With the clinical picture of an autoimmune disorder more clearly evident, her investigations were repeated. Results showed: haemoglobin (Hb) 12.0 g/dL; total leucocyte count (TLC) 7.9 cu/mm; platelet count 2.12 lakh; ESR 40 mm/hr; urea 26 mg/dL; creatinine 0.9 mg/dL; 24-hr urinary protein 266 mg/day (normal < 140 mg/day); bilirubin 0.5 mg/dL; serum glutamic oxaloacetic transaminase (SGOT) 29 IU/L; serum glutamic pyruvic transaminase (SGPT) 18 IU/L; alkaline phosphatase (ALP) 92 IU/L; CRP 3.13 mg/L (normal 0.3–1.0 mg/dL); procalcitonin 18.0 (normal < 0.1 ng/mL); complement component 3 (C3) 90 mg/dL (90–180 mg/dL); complement component (C4) 39 mg/dL (10-40 mg/dL); anti-thyroid peroxidase antibody (anti-TPO Ab) 65.0 IU/mL (normal < 60 IU/mL); TSH: 2.73 µU/mL (normal 0.35 4.94 µU/mL); RF 2.25 (normal < 20 U/mL), ANA titre > 1:1280 homogeneous and speckled; anti-double-stranded deoxyribonucleic acid antibody (anti-dsDNA) > 5 IU/mL (normal < 10 IU/mL); Ro/Sjögren’s syndrome-related antigen A antibody (Ro/SSA) 60 U/mL (normal < 7 U/mL). Based on clinical and laboratory findings, a diagnosis of SLE with Sjögren syndrome was established, and immunomodulatory therapy (hydroxychloroquine 400 mg/day, prednisolone 20 mg/day, mycophenolate 1 g/day) was initiated. Symptoms started resolving within 2–3 months. At 1-year follow-up, the patient was asymptomatic, and her breasts had reduced to near normal size (Figure 3).
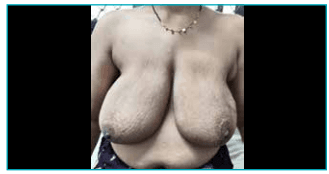
Figure 3: One year after delivery, showing near-complete resolution of gigantomastia following remission of autoimmune disease.
Clinical timeline
The chronological sequence of clinical events, investigations, and outcomes in the present case is summarised in Table 1.
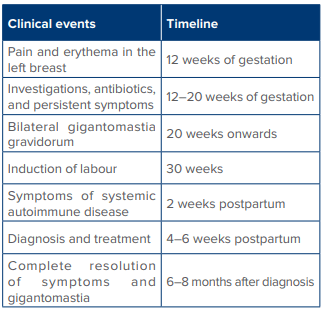
Table 1: Clinical timeline summarising the presentation,investigations, management, and outcome of a patient with autoimmune mastitis and gigantomastia gravidorum progressing to systemic lupus erythematosus with Sjögren’s syndrome.
Discussion
The diagnosis of autoimmune mastitis and GG may be difficult in the early stage and may be confused with inflammatory carcinoma of the breast, especially if it is unilateral. Bilateral axillary swelling due to hypertrophy of the accessory axillary breast tissue may be confused with lymphadenopathy of malignancy.9 However, underlying malignancy should always be considered and excluded first, as there are case reports where patients initially presenting with GG later proved to have underlying malignancy.10,11 Other differential diagnoses, such as a phyllodes tumour, non-Hodgkin’s lymphoma and lymphoblastic lymphoma, can be excluded through biopsy. Biopsy in autoimmune inflammation of the breast may show pathological changes such as: (i) lymphocytic infiltrates; (ii) ductal ectasia; (iii) granulomatous mastitis; and (iv) vasculitis. Although these patterns are not specifically related to a particular autoimmune disease, they provide an indication for a diagnostic pathway.1 Histological features of GG include significant lobular hypertrophy, ductal proliferation, periductal fibrosis, and pseudoangiomatous hyperplasia. In the present case, investigations revealed only subtle changes of chronic perivascular inflammation in skin biopsy with raised inflammatory markers, though autoantibody titres were normal. Pregnancy is known to cause flaring up of autoimmune diseases.12 This may lead to several pregnancy-related complications such as foetal loss, pre-eclampsia and eclampsia, congenital heart block, and neonatal lupus. Spinillo et al. reported that 25% of patients experience a significant rheumatic disease flare during pregnancy.12 Many changes are known to occur within the immune system during pregnancy, such as stimulation of immune cells and release of inflammatory mediators. Mild titres of ANA in normal pregnancy have been variously reported to range from 1%–53%.7 The mechanism by which autoimmune diseases cause inflammation in the breast and gigantomastia is based on a hypothesis that ANA causes an inflammation in the breast that leads to an abnormal proliferation of glandular tissue. However, no specific antibody against a breast antigen has been identified so far. In this patient, a poor obstetric history, perivascular dermal inflammation on breast skin biopsy, and inflammatory markers were some clues towards the autoimmune nature of her problem. There are no clear management guidelines for autoimmune mastitis or GG owing to a huge variability in aetiology and course of the disease. While symptomatic treatment should be offered for autoimmune inflammation, medication with dopamine agonists or surgical intervention are the options for GG, and are employed on a case-by-case basis. A large majority of reports mention the use of surgical procedures in the form of reduction mammoplasties or subcutaneous mastectomies.6,13 Spontaneous complete resolution is a rarity.13 Bromocriptine and cabergoline are the most commonly used drugs. Treatment with bromocriptine has been reported to halt breast growth, though it has no apparent effect on reducing breast size. Both bromocriptine and cabergoline have been shown to have a good safety profile when administered during early pregnancy. Data on exposure of the foetus or embryo to cabergoline during the first weeks of pregnancy have now been reported in more than 900 cases, which indicate that cabergoline is safe in this context.14 Surgical procedures in the form of reduction mammoplasty or bilateral mastectomy with reconstruction are more often employed in the management of GG.13 As a patient can have a relapse after breast-conserving surgery in her future pregnancies, mastectomy is recommended for patients who have not completed their families.15 In a review of 50 cases of GG, 37 cases (74%) were managed surgically, nine received bromocriptine, while two cases had spontaneous resolution in the postpartum period.6 Even though literature does not recommend a conservative approach in patients of GG with an underlying autoimmune condition per se, experience with our case provides some evidence that in patients with autoimmune aetiology of GG, a conservative approach may be adopted with the hope of complete resolution once the disease goes into remission.
Declarations
Conflict of Interests:
The authors declare that there is no conflict of interest regarding the publication of this article.
Funding:
None.
Consent for publication:
Written informed consent was obtained from the patient for the publication of her case report.
Ethical approval:
Ethical approval is not required to publish an anonymous case report.
The diagnosis of autoimmune mastitis and GG may be difficult in the early stage and may be confused with inflammatory carcinoma of the breast, especially if it is unilateral. Bilateral axillary swelling due to hypertrophy of the accessory axillary breast tissue may be confused with lymphadenopathy of malignancy.9 However, underlying malignancy should always be considered and excluded first, as there are case reports where patients initially presenting with GG later proved to have underlying malignancy.10,11 Other differential diagnoses, such as a phyllodes tumour, non-Hodgkin’s lymphoma and lymphoblastic lymphoma, can be excluded through biopsy. Biopsy in autoimmune inflammation of the breast may show pathological changes such as: (i) lymphocytic infiltrates; (ii) ductal ectasia; (iii) granulomatous mastitis; and (iv) vasculitis. Although these patterns are not specifically related to a particular autoimmune disease, they provide an indication for a diagnostic pathway.1 Histological features of GG include significant lobular hypertrophy, ductal proliferation, periductal fibrosis, and pseudoangiomatous hyperplasia. In the present case, investigations revealed only subtle changes of chronic perivascular inflammation in skin biopsy with raised inflammatory markers, though autoantibody titres were normal. Pregnancy is known to cause flaring up of autoimmune diseases.12 This may lead to several pregnancy-related complications such as foetal loss, pre-eclampsia and eclampsia, congenital heart block, and neonatal lupus. Spinillo et al. reported that 25% of patients experience a significant rheumatic disease flare during pregnancy.12 Many changes are known to occur within the immune system during pregnancy, such as stimulation of immune cells and release of inflammatory mediators. Mild titres of ANA in normal pregnancy have been variously reported to range from 1%–53%.7 The mechanism by which autoimmune diseases cause inflammation in the breast and gigantomastia is based on a hypothesis that ANA causes an inflammation in the breast that leads to an abnormal proliferation of glandular tissue. However, no specific antibody against a breast antigen has been identified so far. In this patient, a poor obstetric history, perivascular dermal inflammation on breast skin biopsy, and inflammatory markers were some clues towards the autoimmune nature of her problem. There are no clear management guidelines for autoimmune mastitis or GG owing to a huge variability in aetiology and course of the disease. While symptomatic treatment should be offered for autoimmune inflammation, medication with dopamine agonists or surgical intervention are the options for GG, and are employed on a case-by-case basis. A large majority of reports mention the use of surgical procedures in the form of reduction mammoplasties or subcutaneous mastectomies.6,13 Spontaneous complete resolution is a rarity.13 Bromocriptine and cabergoline are the most commonly used drugs. Treatment with bromocriptine has been reported to halt breast growth, though it has no apparent effect on reducing breast size. Both bromocriptine and cabergoline have been shown to have a good safety profile when administered during early pregnancy. Data on exposure of the foetus or embryo to cabergoline during the first weeks of pregnancy have now been reported in more than 900 cases, which indicate that cabergoline is safe in this context.14 Surgical procedures in the form of reduction mammoplasty or bilateral mastectomy with reconstruction are more often employed in the management of GG.13 As a patient can have a relapse after breast-conserving surgery in her future pregnancies, mastectomy is recommended for patients who have not completed their families.15 In a review of 50 cases of GG, 37 cases (74%) were managed surgically, nine received bromocriptine, while two cases had spontaneous resolution in the postpartum period.6 Even though literature does not recommend a conservative approach in patients of GG with an underlying autoimmune condition per se, experience with our case provides some evidence that in patients with autoimmune aetiology of GG, a conservative approach may be adopted with the hope of complete resolution once the disease goes into remission.
Conclusion:
Autoimmune mastitis should be considered as a differential diagnosis in patients with persistent inflammation of the breast, while adequately investigating the patient to rule out a malignancy. GG has a chance for complete remission when the autoimmune disease goes into remission.
Navneet Kaur, Virali Savani. Autoimmune Mastitis with Gigantomastia Gravidorum: Report of a Case and
Review of Literature. MMJ. 2026,
March. Vol 3 (1).
References
- Goulabchand R, Hafidi A, Van de Perre P, et al. Mastitis in Autoimmune Diseases: Review of the Literature, Diagnostic Pathway, and Pathophysiological Key Players. J Clin Med.2020;9(4):958.
- Rosa M, Mohammadi A. Lupus mastitis: A review. Ann Diagn Pathol. 2013;17(2):230–3.
- Fong D, Lann MA, Finlayson C, et al. Diabetic (lymphocytic)mastopathy with exuberant lymphohistiocytic and granulomatous response: A case report with review of the literature. Am J Surg Pathol. 2006;30:1330–6.
- Meislin HW, Iserson KV, Kaback KR, et al. Airway trauma.Emerg Med Clin North Am. 1983;1(2):295-312.
- Antevski BM, Smilevski DA, Stojovski MZ, et al. Extreme gigantomastia in pregnancy: case report and review of literature. Arch Gynecol Obstet. 2007;275:149–53.
- Dancey A, Khan M, Dawson J. Gigantomastia a classification and review of the literature. J Plast Reconstr Aesthet Surg.2008;61:493–502.
- Mangla M, Singla D. Gestational gigantomastia: a systematic review of case reports. J Midlife Health. 2017;8:40–4.
- Zingaretti N, De Biasio F, Riccio M, et al. A case of gestational gigantomastia in a 37-years-old woman associated with elevated ANA: a casual linkage? Pan Afr Med J. 2017;27:167.
- Touraine P, Youssef N, Alyanakian MA, et al. Breast inflammatory gigantomastia in a context of immune-mediated diseases. J Clin Endocrinol Metab. 2005;90:5287–94.
- Ezem BU, Osuagwu CC, Opara KA. Gestational gigantomastia with complete resolution in a Nigerian woman. BMJ Case Rep.2011:bcr01201026322011.
- Vandenberghe G, Claerhout F, Amant F. Lymphoblastic lymphoma presenting as bilateral gigantomastia in pregnancy.Int J Gynaecol Obstet 2005;91:252–3.
- Windom KW, McDuffie RS Jr. Non‑Hodgkin’s lymphoma presenting with gigantomastia in pregnancy. Obstet Gynecol.1999:93(5 Pt 2);852.
- Spinillo A, Benvenuti F, Epis OM, et al. The effect of newly diagnosed undifferentiated connective tissue disease on pregnancy outcome. Am J Obstetrics Gynecol. 2008;199:632e1–e6.
- Alhindi N, Mortada H, Alzaid W, et al. A Systematic Literature Review of the Clinical Presentation, Management, and Outcome of Gestational Gigantomastia in the 21st Century. Aesthetic Plast Surg. 2023;47(1):10–29.
- Maiter D. Prolactinoma and pregnancy: From the wish of conception to lactation. Ann Endocrinol (Paris).2016;77(2):128–34.
- Türkan H, Gökgöz MŞ, Taşdelen İ, et al. Gestational Gigantomastia. J Breast Health. 2016;12(2):86–7.