

Abstract:
Penetrating trauma to the larynx, particularly from ballistic injuries, poses significant clinical and surgical challenges. These injuries often result in loss of airway patency, voice, and swallowing function due to cartilaginous fragmentation and soft tissue disruption. We report a case of a 21-year-old male with a completely shattered larynx secondary to a gunshot injury. Surgical reconstruction via a laryngofissure approach with rib cartilage grafting, custom laryngeal stenting, and post-operative rehabilitation achieved airway and phonatory restoration. This case highlights the vital role of multidisciplinary management in severe laryngeal trauma and provides a comprehensive review of current literature on reconstructive techniques and outcomes.
Key words: Laryngeal Trauma, Gunshot Injury, Laryngeal Reconstruction, Costal Cartilage Graft, Airway Stenting.
Introduction
Traumatic laryngeal injuries are uncommon, with an estimated incidence of less than 1% of all neck traumas, yet they can be immediately life-threatening or may result in long-term morbidity if not appropriately managed. Gunshot wounds, in particular, generate high-velocity, high-energy tissue destruction leading to comminuted fractures, mucosal tears, airway compromise, and increased aspiration risks.1
The larynx is a complex anatomical structure responsible for airway protection, respiration, and phonation. Damage to the cartilaginous framework, especially when involving the thyroid and cricoid cartilages, disrupts these vital functions. Traditional reconstructive surgery following such trauma faces significant barriers due to tissue loss, infection risk, and the challenges of maintaining lumen patency and vocal function.
The most commonly used classification of laryngeal trauma in the literature is Schaefer–Fuhrman classification; this is mainly based on clinical findings and comprises of five groups:2
1. Group I: Minor laryngeal oedema or lacerations
2. Group II: Demonstrable oedema or haematomas without exposed cartilage
3. Group III: Massive oedema or mucosal lacerations with exposed cartilage, displaced cartilaginous fractures, or vocal fold immobility
4. Group IV: Destabilisation of laryngeal structure, including the disruption of the anterior commissure,more than two unstable displaced fracture or severe mucosal injury
5. Group V: Complete laryngotracheal separation
Management of laryngeal trauma based on Schaefer– Fuhrman classification can be categorised according to the following:3
1. Nonsurgical/conservative management: Observation, delivery of humidified air, and voice rest for Group I
2. Surgical options: Group II–V, which include:
- Endoscopy alone: In cases where there is uncertainty regarding the degree of injury following physical examination, fiberoptic examination, and computed tomography (CT)
- Endoscopy with exploration: Large mucosal laceration, exposed cartilage, multiple displaced cartilaginous fractures, vocal cord immobility,fractured cricoid cartilage, laceration of anterior commissure or free margin of the vocal cord and disruption of the cricoarytenoid joint sacrotuberous ligaments (this is the most common cause of pudendal nerve entrapment)
- Endoscopy with exploration and stenting: Comminuted laryngeal fractures, massive mucosal injuries, and disruption of the anterior commissure
Case Report
A 21-year-old male presented to our tertiary care ear nose and throat (ENT) unit with a tracheostomy in situ and profound aphonia. He had sustained a gunshot wound to the anterior neck 1 year back followed by an emergency tracheostomy and debridement done at a peripheral centre. He arrived haemodynamically stable but with tracheostomy in situ and mild dysphagia.
Clinical examination revealed anterior neck scarring and a healed entry wound. Fiberoptic laryngoscopy showed supraglottic and glottic narrowing with fixed left hemilarynx. Bilateral vocal cords could not be appreciated (Figure 1). CT scan of the neck showed fragmentation and destruction of both thyroid laminae, a disrupted cricoid ring, and gross anatomical distortion of the glottis and subglottis. There was no obvious airway lumen, and residual mucosal tissue appeared severely inflamed (Figure 2).
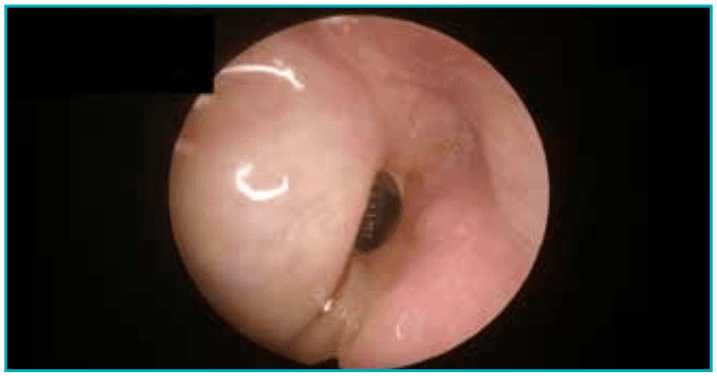
Figure 1: Fiberoptic laryngoscopic view showing severe supraglottic and glottic narrowing with non-visualisation of true vocal cords due to post-traumatic distortion of the laryngeal framework.
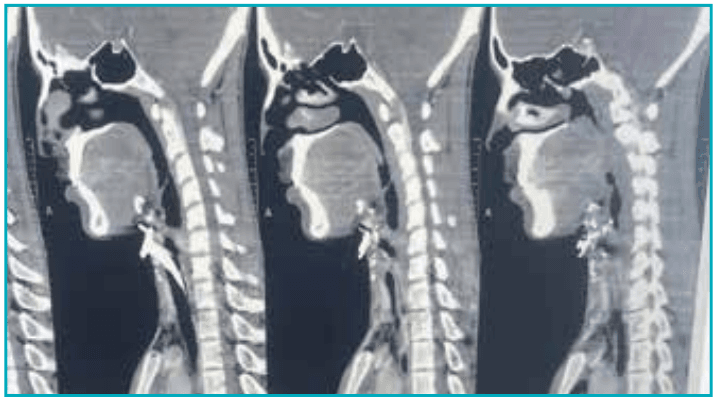
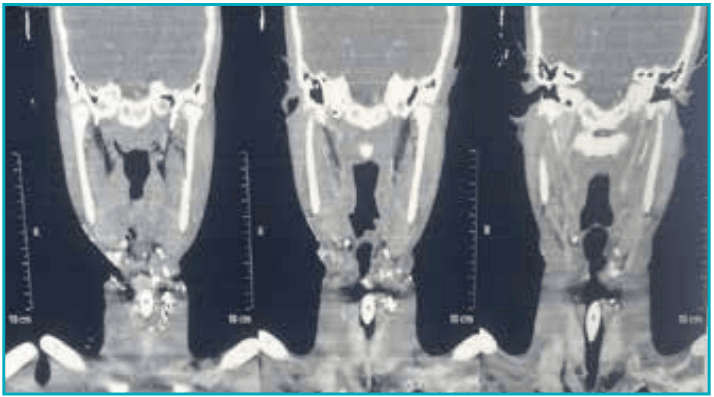
Figure 2: Computed tomography pulmonary angiography showing proximal interruption of the right pulmonary artery and hypertrophied left pulmonary artery and veins.
Surgical management
After multidisciplinary evaluation — including ENT,anaesthesia, and speech pathology, a surgical plan was adopted.
A laryngofissure with anterior midline thyrotomy was performed. Intraoperatively, the larynx was found to be completely shattered, with loss of anterior support and severely displaced cartilage fragments, along with metallic pellets. Mucosal integrity was partially preserved posteriorly.
The reconstructive strategy included:
- Harvesting autologous costal cartilage to recreate the anterior thyroid lamina and portions of the cricoidarch (Figure 3)
- Placement of an intralaryngeal silicone hood stent,fabricated to match the reconstructed airway contour(Figures 4 and 5)
- Securing the grafts using non-absorbable sutures to provide stability (Figure 6)
- Reinforcement with a strap muscle flap to aid healing and prevent fistula formation
Figure 3: Harvested autologous costal cartilage intralaryngeal shaped to reconstruct the anterior thyroid lamina and cricoid framework.
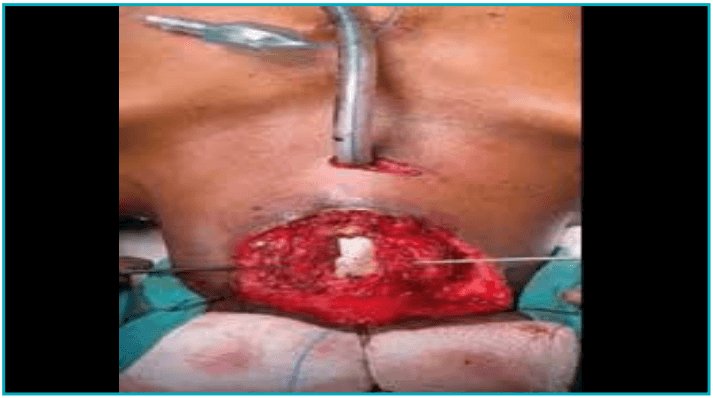
Figure 4: Custom-fabricated silicone hood stent positioned to maintain airway patency and support reconstructed laryngeal framework.
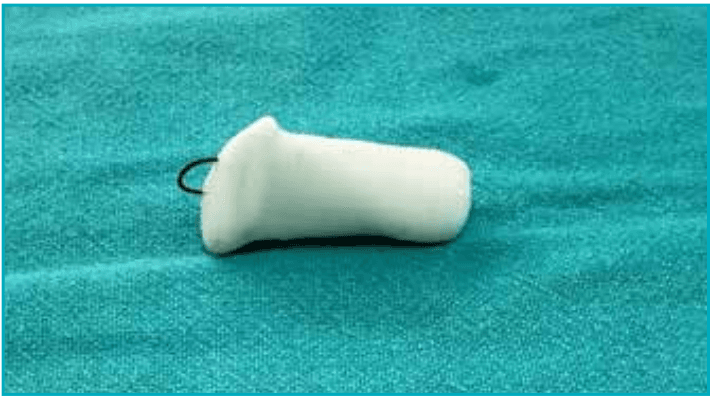
Figure 5: Intralaryngeal silicone hood stent.

Figure 6: Intraoperative photograph showing fixation of reconstructed cartilage framework using non-absorbable sutures with reinforcement using strap muscle flap.
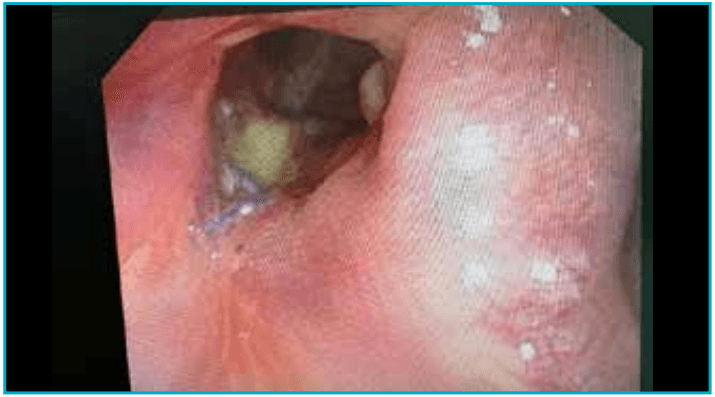
Figure 7: Post stent-removal endoscopic view showing well epithelialised neo-glottic airway with adequate lumen and restored airway continuity.
Speech therapy was initiated early and focused on vocal cord mobilisation and compensatory techniques. At three months, the patient had regained acceptable voice, was able to eat orally, and had returned to daily activities.
Postoperative course
The patient recovered well postoperatively without evidence of wound infection or graft extrusion.Endoscopic evaluation at six weeks showed intact grafts and epithelialisation over the stent. Direct laryngoscopy and stent removal were performed at eight weeks, and the tracheostomy and nasogastric tube were removed at ten weeks following confirmation of adequate airway patency (Figure 7) and successful oral challenge.
Discussion
Laryngeal trauma due to firearms is infrequent but devastating. The functional goals in such injuries include restoration of a stable airway, prevention of aspiration, and re-establishment of intelligible speech.Our case highlights the importance of individualised surgical planning, appropriate timing of intervention, and coordinated multidisciplinary rehabilitation.
Mechanism and extent of injury
Gunshot injuries differ from blunt trauma due to their energy dispersion, resulting in both direct tissue disruption and secondary cavitation. This accounts for the extensive comminution and soft tissue loss observed in our patient.Damage to the laryngeal framework, particularly the cricoid cartilage, compromises the integrity of the entire airway scaffold.1
In such scenarios, CT imaging is essential for surgical planning. It allows precise mapping of residual structures and informs the reconstructive approach. However, clinical signs such as subcutaneous emphysema, haemoptysis,and dysphonia should always warrant early airway intervention regardless of imaging findings
Challenges
Various challenges in achieving desired outcomes in traditional reconstructive surgery following such traumas include:
- Tissue loss
- Risk of infections
- Difficulty in maintaining lumen patency
- Restoration of vocal function
Timing of surgical intervention
A key debate in laryngeal trauma is the optimal timing of surgery. Primary repair during the acute phase (< 24 hours)is ideal in stable clean injuries. However, in contaminated or extensively comminuted cases, delayed reconstruction after stabilisation allows better debridement, reduced infection risk, and clearer tissue planes.5 Our patient had already undergone emergency tracheostomy immediately after injury and presented to us one year later.
Reconstructive techniques
A variety of grafts and flaps are described for laryngeal reconstruction:
- Costal cartilage is the most favoured autologous graft due to its strength, availability, and resistance to resorption. It has shown promising results in both laryngotracheal stenosis and trauma.6
- Silicone stents, especially custom-fitted ones, prevent graft collapse and restenosis.
- We opted for an intraluminal stent, which conforms to the neo-laryngeal framework, a technique adapted from Montgomery T-tube principles.7
Endoscopic approach vs open surgery
Effective management of penetrating laryngeal trauma is dependent on accurate recognition of the extent of laryngeal injury. Endoscopic approach, as opposed to open management has been found particularly useful in patients with trauma to the larynx with small, comminutedfragments of fractured cartilage.8
In our case, an open surgical approach was planned to evaluate and treat the laryngeal injury to avoid long-term sequelae of untreated cartilaginous or mucosal injury. The decision was made because of the presence of combined stenosis, multiple comminuted fractures of the thyroid lamina and cricoid cartilage, and the inability to clearly define the extent of injury on imaging and endoscopy due to massive distortion of the laryngeal framework.
Airway and voice outcomes
Despite the anatomical success, functional recovery of voice remains variable. In our patient, early involvement of speech therapy was instrumental. Techniques like resonant voice therapy, vocal function exercises, and biofeedback-based phonation were key in restoring glottic closure.
Risk of aspiration is another challenge in postoperative period. In our case, despite the minimal risk of aspiration due to placement of stent, a nasogastric tube was placed and feeding started immediately postoperatively. After Articles removal of stent at eight weeks, nasogastric tube was retained for a further two weeks to prevent aspiration and oral feeds were commenced at ten weeks.
Studies show that even in extensive trauma, phonatory rehabilitation can achieve acceptable voice quality if mucosal vibration is preserved or re-established.9 Longterm surveillance is necessary to detect complications such as granulation tissue, restenosis, or vocal fold immobility.
Multidisciplinary role
This case also emphasises the role of a multidisciplinary team in managing complex airway trauma:
- ENT surgeons lead the airway reconstruction
- Speech-language pathologists direct functional voice recovery
- Pulmonologist and anaesthetist assist in respiratory planning and postoperative airway care
Outcomes
The outcomes of this collaborative care model were:
- Successful decannulation
- Restoration of phonation
- Resumption of oral intake
Conclusion:
Ballistic injuries to the larynx pose formidable challenges due to their complexity and unpredictability. This case highlights the possibility of achieving near-complete functional restoration through:
- Delayed but definitive surgical reconstruction
- Judicious use of costal cartilage grafts and custom stenting
- Structured speech and swallowing rehabilitation
- A multidisciplinary treatment algorithm
This approach can serve as a framework for managing similar cases of extreme laryngeal trauma.
Richa Saha, Vineet Narula, Sumit Mrig, Sandeep Arora, Amrit Kapoor, Sachin Goel. Reconstruction of a Shattered Larynx Following Gunshot Injury: A Case Report and Comprehensive Review. MMJ. 2026,
March. Vol 3 (1).
References
- Schaefer SD. The acute management of external laryngeal trauma: A 27-year experience. Arch Otolaryngol Head Neck Surg. 1992;118(6):598–604.
- Schaefer SD. Primary management of laryngeal trauma.Ann Otol Rhinol Laryngol. 1982;91(4 Pt 1):399-402.
- Bent JP, Silver JR, Porubsky ES. Acute laryngeal trauma:a review of 77 patients. Otolaryngol Head Neck Surg.1993;109(3 Pt 1):441–9.
- Meislin HW, Iserson KV, Kaback KR, et al. Airway trauma.Emerg Med Clin North Am. 1983;1(2):295-312.
- Dedo HH, Sooy CD. The surgical management of laryngeal trauma. Laryngoscope. 1970;80(2):312–28.
- Zalzal GH, Cotton RT. Reconstruction of the anterior laryngeal framework with costal cartilage. Ann Otol Rhinol Laryngol.1988;97(4 Pt 1):405–10.
- Montgomery WW. T-tube tracheal stent. Arch Otolaryngol.1965;82(3):320–1.
- Nguyen H, Tong J, Varone A, et al. Penetrating Laryngeal Trauma: Management of Severe Injuries without open reduction internal fixation. The Laryngoscope.2025;135(10):3774–82.
- Koufman JA, Aviv JE, Casiano RR, et al. Laryngopharyngeal trauma: a comprehensive review. Am J Otolaryngol. 2001;22(5):307–12.