

Abstract:
Histoplasmosis is a systemic fungal infection caused by Histoplasma capsulatum, commonly seen in immunocompromised or elderly individuals with environmental exposure. A 65-year-old male taxi driver from Gurugram, with a history of diabetes mellitus and hypertension, presented with a 10-day history of highgrade fever, nausea, anorexia, weakness, and unintentional weight loss. Laboratory investigation showed anaemia (haemoglobin [Hb] 9.2 g/dL), hyponatraemia (sodium [Na] 123.7 mEq/L), elevated liver enzymes (alkaline phosphatase [ALP] 576 U/L, gamma-glutamyl transferase [GGT] 207 U/L), hypoalbuminaemia, and markedly raised C-reactive protein (CRP) 157.7 mg/L. Imaging revealed right middle zone consolidation, mild pleural and pericardial effusions, and hepatosplenomegaly. Serological and microbiological tests for dengue, malaria, typhoid, and viral hepatitis were negative. The patient showed partial improvement with antibiotics; however, fever recurred, and bone marrow aspiration (BMA) demonstrated intracellular yeast-like organisms morphologically consistent with H. capsulatum.
Key words: Histoplasmosis, Histoplasma capsulatum, Seizures, Liposomal Amphotericin B, Itraconazole.
Introduction
Histoplasmosis is a global disease, endemic to regions across all six inhabited continents. Most epidemiological research on histoplasmosis has been conducted in the United States, where the infection has a broad geographic distribution. Recent syntheses of multiple studies have demonstrated a scattered global distribution of histoplasmosis, with case series reported from Brazil, South Africa, and India, and isolated cases documented in Central and South America, northern sub-Saharan Africa, Oceania, and Europe.1 Although Randhawa's 1970 review identified 30 autochthonous cases of histoplasmosis in Southeast Asia, the epidemiology of this fungal infection in the region has remained relatively unexplored.2
Histoplasmosis is a systemic fungal infection caused by Histoplasma capsulatum, a dimorphic fungus commonly found in soil3 contaminated with bird or bat droppings. The disease is endemic in certain regions, particularly river valleys and areas with high humidity. Infection occurs primarily through inhalation of fungal spores, which convert to the yeast form within the lungs and may subsequently disseminate throughout the body, especially in immunocompromised individuals.4,5
In India, histoplasmosis cases are likely underdiagnosed and under-reported, although areas of high prevalence include the eastern states of West Bengal and Assam, through which the Ganges3 and Brahmaputra rivers flow. Areas outside these traditional riverine foci, including several eastern and northern states such as Bihar,Delhi, Haryana, Rajasthan, Punjab, and Uttar Pradesh, have also documented cases.6 India may therefore represent a region of substantial underdiagnosis.7 In this study, five individuals, residing in the eastern part of India, were identified with histoplasmosis between December 2022 and April 2024. Notably, all patients were human immunodeficiency virus (HIV)-negative but had underlying comorbidities such as diabetes or renal impairment. While many infections remain asymptomatic or self-limiting, histoplasmosis can present with a wide spectrum of clinical manifestations ranging from mild respiratory illness8 to severe disseminated disease. Due to its nonspecific symptoms and resemblance to other pulmonary or systemic diseases such as tuberculosis, diagnosis is often challenging and delayed. Early recognition and appropriate antifungal therapy are crucial to prevent complications and improve patient outcomes.
This case study reports the clinical presentation, diagnostic challenges, and management of a patient diagnosed with histoplasmosis, highlighting the importance of considering fungal infections in the differential diagnosis of chronic or unexplained febrile illnesses.
Case Report
A 65-year-old male taxi driver from Gurugram, with a 20-year occupational history involving environmental exposure and known comorbidities of diabetes mellitus and hypertension under moderate control, presented with a 10-day history of intermittent moderate- to high-grade fever, increased urinary frequency, loss of appetite, generalised weakness, and unintentional weight loss. His oral intake had declined, and he felt too weak to even go to the washroom unaided. He had previously been admitted to a nursing home for 7 days, where he received intravenous (IV) antibiotics and supportive care, but showed no clinical improvement. On examination, the patient appeared dehydrated, anaemic, and icteric, with abdominal distension and right lower lobe crepitations. Laboratory investigations revealed anaemia (haemoglobin [Hb] 9.2 g/dL), hyponatraemia (sodium [Na] 123.7 mEq/L), elevated liver enzymes (alkaline phosphatase [ALP] 576 U/L, gammaglutamyl transferase [GGT] 207 U/L), hypoalbuminaemia (2.8 g/dL), and elevated C-reactive protein (CRP)(157.7 mg/L). Serological tests for dengue, malaria, typhoid, and viral hepatitis were negative.
X-ray image
Chest X-ray and computed tomography (CT) thorax showed bilateral mild pleural effusion with right middle zone consolidation and minimal pericardial effusion. Ultrasonography revealed hepatosplenomegaly. The patient showed partial improvement after 7 days of antibiotic therapy. Based on his clinical condition, he was discharged on cefotaxime (Monocef) and azithromycin (Azee), with advice to follow up. At review, he reported ongoing anorexia and weakness, despite discontinuing his oral hypoglycaemic agents (OHAs). The essential blood profile showed mild improvements.
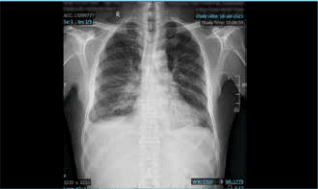
Figure 1: Chest X-ray (Posteroanterior [PA] view) showing prominent bronchovascular markings with inhomogeneous haziness and fibrotic opacities in the bilateral lower lung zones.Blunting of the right costophrenic angle suggests a right-sided pleural effusion.
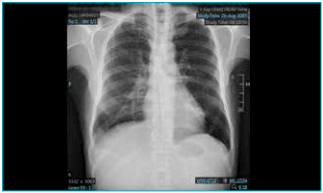
Figure 2: Follow-up chest X-ray (Posteroanterior [PA] view)demonstrating interval resolution of pleural effusion with mild residual prominence of bronchovascular markings. Cardiac silhouette and mediastinal contours are normal. Nearly one month later, the patient presented with acute neurological symptoms (generalised tonic clonic seizures [GTCS] and unconsciousness) alongside a protracted fever of unknown origin (FUO). Extensive investigations revealed significant systemic pathology,including sepsis, pneumonia, biventricular effusions(pleural and pericardial), pancytopenia (anaemia,leukopenia, thrombocytopenia), electrolyte imbalance,and immune suppression (CD4 count 138.56/μL)Bone marrow findings reassuringly excluded acute leukaemia, suggesting the cytopenias were likely secondary to overwhelming systemic illness (sepsis, chronic disease, nutritional deficits).
Bone marrow report image
Bone marrow aspiration subsequently demonstrated intracellular yeast-like organisms morphologically consistent with H. capsulatum (Figure 3A and 3B). The patient was commenced on liposomal amphotericin B (3–5mg/kg IV daily for 1–2 weeks), followed by step-down therapy with itraconazole (200 mg three times daily for 3 days, then 200 mg twice daily for 12 weeks). Followup phase showed slow but consistent improvement across all parameters.
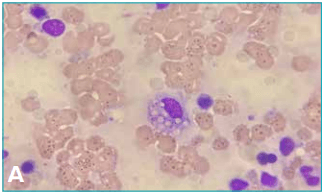
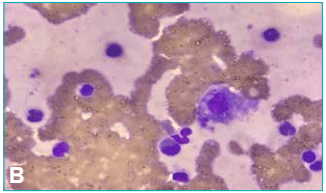
Figure 3: A, B. Bone marrow aspiration stains showing ringlike structures within white blood cell cytoplasm, suggestive of histoplasmosis.
Medications for histoplasmosis
Severe cases: Treatment with IV amphotericin B.
Mild to moderate cases: Treatment often begins with itraconazole.
Follow-up therapy: After initial treatment for severe cases, itraconazole was continued as maintenance therapy to prevent relapse. Fluconazole, voriconazole, posaconazole, and isavuconazole may be used as alternatives, particularly for patients with contraindications or side effects to amphotericin B or itraconazole.
Duration: Treatment duration depends on disease severity and the patient’s immune status and may extend to one year or longer.
Antiretroviral therapy (ART): For patients with HIV, ART should be started immediately to improve outcomes and support immune recovery.
Relapse risk - Non-adherence to treatment. Prophylaxis: Itraconazole prophylaxis may be used to prevent histoplasmosis in patients with severely compromised immune systems (CD4 counts < 100/µL) during outbreaks.
Discussion
H. capsulatum was first discovered in 1905 by Samuel T. Darling, but only in the 1930s was it recognised as a widespread infection. H. capsulatum is a dimorphic fungus that exists as a mould in the environment and as yeast-like structures with septate hyphae at 37°C in tissues.9 Human infection occurs following inhalation of the fungus (in the form of microconidia or hyphal fragments), which reaches the alveoli and transforms into the yeast phase. Most infected individuals remain asymptomatic, but symptomatic patients face a substantial risk of mortality and severe morbidity depending on the host's immune status.
Disseminated histoplasmosis is an opportunistic fungal infection caused by H. capsulatum, typically seen in immunocompromised or elderly individuals. Histoplasma can also exist inside the host in a latent form with the potential for reactivation.5 Histoplasmosis is often difficult to diagnose because its symptoms are similar to many other illnesses. This fungal infection can mimic community-acquired pneumonia,4 tuberculosis, lymphoma, sarcoidosis, and cancer.5
The patient presented in this case study, with a background of diabetes mellitus, presented with prolonged fever, hepatosplenomegaly, weight loss, and pulmonary involvement, raising suspicion for disseminated fungal infection. The seizure was likely provoked by the severe systemic illness (sepsis, electrolyte imbalance, or fever). The significant immune suppression is a major concern and likely contributed to the development of multiple infections, including the fungal esophagitis. The coexistence of cardiac (left ventricular failure [LVF]) and hepatic dysfunction (chronic liver disease [CLD]) complicates management and could contribute to the effusions and hypoproteinaemia. Bone marrow examination confirmed histoplasmosis, explaining the systemic symptoms and multi-organ involvement. Pleural and pericardial effusions likely resulted from inflammatory and infective processes secondary to dissemination. Histoplasma causing hemophagocytic lymphohistiocytosis (HLH) is a severe complication and is associated with high mortality.11 This is caused by uncontrolled activation of the T cell, resulting in a cytokine storm. The clinical features of HLH mimic that of severe sepsis, and thus, HLH may be missed in the setting of an overwhelming infection.
Histoplasmosis is common along the Mississippi and Ohio river valleys. Only 27% of infectious disease physicians (IDP) observed histoplasmosis outside these endemic areas.4 The Infectious Diseases Society of America (IDSA) guidelines for the management of histoplasmosis were revised 15 years ago. In a survey, only 46% (253/551) of respondents were patients with histoplasmosis. In regions considered endemic, 82% (158/193) of physicians reported histoplasmosis cases, compared with 27% (95/358) in regions not classically considered endemic (p < 0.001).4.13 In Max Hospital laboratory, around 6 cases have been reported so far, as shared by the pathologist.
Most IDP follow IDSA treatment guidelines, recommending itraconazole6 for acute pulmonary7 histoplasmosis (189/253 [75%]), mild-to-moderate disseminated disease (189/253 [75%]), and as stepdown therapy for severe disseminated histoplasmosis with (232/253 [92%]) or without (145/253 [57%]) central nervous system involvement. No consensus recommendations were observed for survey questions regarding immunocompromised patients.
A timely diagnosis requires a high index of clinical suspicion by clinicians. Clinicians often rely on a history of exposure to areas considered endemic for Histoplasma, such as the Ohio and Mississippi river valleys. Despite substantial evidence of its global presence, Histoplasma is still regarded by many as predominantly endemic to specific regions of North America.4,8 This perception can result in clinicians failing to consider histoplasmosis on a differential diagnosis, contributing to delayed diagnosis and poor outcomes.
IDSA last updated clinical guidelines for the management of histoplasmosis in 2007, using literature from 1st January 1999 through 31st June 2006.3 Since the release of the guidelines, new treatment options have been developed. Posaconazole was approved by the United States Food and Drug Administration (US-FDA) shortly before the release of the 2007 guidelines, and isavuconazole was approved in 2015. Both maintain in vitro activity against Histoplasma even in the setting of fluconazole resistance,5,10 though there are limited clinical data to support their use in treating histoplasmosis.11-12 Since the arrival of these new medications, there have been no changes to clinical practice recommendations,13 and very little new data have been published to guide therapy. Additionally, the population at risk of developing clinically significant histoplasmosis has increased substantially, with millions of patients receiving an ever-expanding variety of immunosuppressive medications and/or living with immunosuppressive medical conditions.
Conclusion:
The present case illustrates how disseminated histoplasmosis can mimic other systemic illnesses, highlighting the need for clinical vigilance, timely diagnostic evaluation, and early recognition with prompt antifungal treatment to prevent severe complications and improve patient outcomes.
Rajiv Dang, Krishna Veni, Gaurav Kapoor, Akash Banwari, Sujata Yadav, Nitin Dayal. Histoplasmosis – An Infrequent Cause of Fever. MMJ.
2026, March. Vol 3 (1).
References
- Baker J, Setianingrum F, Wahyuningsih R, et al. Mapping histoplasmosis in Southeast Asia–implications for diagnosis in AIDS. Emerg Microbes Infect. 2019;8(1):1139–45.
- Randhawa HS. Occurrence of histoplasmosis in Asia.Mycopathol Mycol Appl. 1970;41(1):75–89.
- Sanyal M, Thammayya A. Histoplasma capsulatum in the soil of Gangetic plain in India. Indian J Med Res.1975;63(7):1020–8.
- Azar MM, Loyd JL, Relich RF, et al. Current Concepts in the Epidemiology, Diagnosis, and Management of Histoplasmosis Syndromes. Semin Respir Crit Care Med. 2020;41(1):13–30.
- Wheat LJ, Azar MM, Bahr NC, et al. Histoplasmosis. Infect Dis Clin North Am. 2016;30(1):207–27.
- Ashraf N, Kubat RC, Poplin V, et al. Re-drawing the maps for endemic mycoses. Mycopathologia. 2020;185(5):843–65.
- Ray A, Aayilliath KA, Banerjee S, et al. Burden of serious fungal infections in India. Open Forum Infect Dis.2022;9(12):ofac603.
- Sanyal M, Thammayya A. Skin sensitivity to histoplasmin in Calcutta and Its neighbourhood. Indian J Dermatol Venereol Leprol. 1980;46(2):94–8.
- Darling ST. A protozoön general infection producing pseudotubercles in the lungs and focal necroses in the liver, spleen and lymphnodes. JAMA. 1906;46(17):1283–85.
- Kaufmann C. Pathogenesis and clinical manifestations of disseminated histoplasmosis. UpToDate. 2024. Available at: https://www.scribd.com/document/943699396/Pathogenesis-and-Clinical-Manifestations-of-DisseminatedHistoplasmosis-UpToDate. Accessed on: 20th November 2025.
- Paolo WF Jr, Nosanchuk JD. Adrenal infections. Int J Infect Dis. 2006;10(5):343–53.
- Jabr RE, El Atrouni W, Male HJ, et al. HistoplasmosisAssociated Hemophagocytic Lymphohistiocytosis: A Review of the Literature. Can J Infect Dis Med Microbiol. 2019(1):7107326.
- Krishnan G, Power M, Bariola JR, et al. Comparison of indirect fungal diagnostic tests in patients with proven histoplasmosis. Open Forum Infect Dis. 2022;9(11):ofac609.