

Abstract:
Adrenal involvement in histoplasmosis is typically associated with disseminated infection in immunocompromised individuals. Isolated adrenal histoplasmosis in immunocompetent hosts is rare and frequently mimics neoplastic pathology. A 47-year-old immunocompetent male presented with an incidentally discovered 7 cm left adrenal mass. Hormonal evaluation was unremarkable. He underwent robotic adrenalectomy with cholecystectomy for concurrent gallstones. Gross pathology revealed a well-encapsulated adrenal mass with necrosis. Microscopy demonstrated an adrenocortical adenoma with extensive granulomatous inflammation containing numerous intracellular budding yeasts morphologically consistent with Histoplasma capsulatum. The patient had no systemic symptoms of fungal infection. This case highlights the diagnostic challenge posed by unilateral adrenal histoplasmosis in immunocompetent individuals. Histopathology remains essential for diagnosis, particularly when radiologic and biochemical features suggest an adrenal neoplasm. Awareness of this entity is crucial to avoid misdiagnosis and to guide appropriate postoperative management.
Key words: Histoplasmosis, Immunocompetent, Fungal Infection, Adrenal Gland.
Introduction
Histoplasmosis is a systemic fungal infection caused by Histoplasma capsulatum, a dimorphic fungus endemic in several regions worldwide, particularly areas rich in bird and bat guano.1,2Infection typically occurs via inhalation of microconidia, and while pulmonary involvement is most common, dissemination may occur in susceptible hosts. Isolated adrenal histoplasmosis (IAH) in immunocompetent individuals is distinctly uncommon. Most reported cases describe bilateral adrenal enlargement, whereas unilateral disease may mimic an adrenal neoplasm clinically and radiologically.3–5
We report an unusual case of unilateral adrenal histoplasmosis incidentally identified in an immunocompetent adult undergoing adrenalectomy for a presumed cortical neoplasm.
Case Report
A 47-year-old male with no significant past medical, personal, or family history presented with an incidentally detected left adrenal mass measuring 7.0 × 5.0 cm. The lesion was discovered during evaluation for unrelated symptoms. He also had multiple gallstones identified on imaging. He denied fever, weight loss, respiratory symptoms, or features of endocrine dysfunction.
Clinical evaluation
Physical examination was unremarkable. Patient had a history of old malunited pelvic injury with non-union of sacrum and sacral nerves 2–4 (S2–4) nerve injury; for which he underwent open reduction and internal fixation with bone grafting and sacroiliac fixation in the year 2018. 133 The Max Medical Journal March 2026 Computed tomography (CT) findings showed central hypodensity and peripheral enhancement. Functional adrenal evaluation — including serum cortisol, 24-hour urinary free cortisol, urinary vanillylmandelic acid (VMA), aldosterone–direct renin ratio (ARR), 24-hour urinary metanephrine, and dehydroepiandrosterone sulphate (DHEA-S) was within normal limits. These findings effectively excluded pheochromocytoma and other hormonally active adrenal tumours.
A large unilateral adrenal mass suspicious for a neoplasm was identified, leading the surgical team to recommend excision, with a provisional diagnosis of a non-functional adrenocortical adenoma.
Hospital course
The patient underwent left robotic adrenalectomy and cholecystectomy. Intraoperatively, a 7–8 cm left adrenal tumour and gallstones were identified. The postoperative period was uneventful, and the patient was discharged in stable condition on postoperative Day 3 with advice for follow-up after receipt of the histopathology report.
Histopathology
Gross examination of the left adrenal specimen showed dimensions of 11.0 × 9.0 × 5.0 cm and a weight of 180 g. The cut surface revealed a well-encapsulated yellow mass measuring 7.0 × 4.5 × 5.5 cm, with focal areas of necrosis and haemorrhage.
On microscopy, sheets of enlarged cells with distinct cell borders and abundant foamy cytoplasm, resembling zona fasciculata, were observed, along with extensive serpentine areas of necrosis surrounded by granulomatous inflammation (Figure 1A). The inflammatory infiltrate comprised foam cells, multinucleated giant cells, neutrophils, lymphocytes, and plasma cells (Figure 1B). Numerous small (2–5 µm), uniform, oval, budding yeast forms with eccentric nuclei were clustered within histiocytes, morphologically consistent with Histoplasma capsulatum. Periodic acid–Schiff (PAS) and Grocott-Gomori methenamine silver (GMS) stains confirmed the diagnosis of adrenal histoplasmosis Figures 2 and 3.

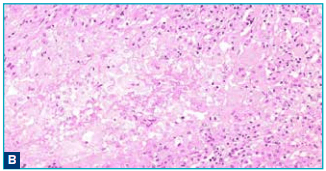
Figure 1: Haematoxylin and Eosin (H&E) stain: A. Tissue section showing extensive areas of serpiginous necrosis with surrounding granulomatous inflammation within the adrenal lesion (H&E, ×10); B. Demonstrating sheets of histiocytes, multinucleated giant cells, and foamy macrophages. Numerous small oval yeast forms are visible within the cytoplasm of histiocytes. (H&E, ×10).
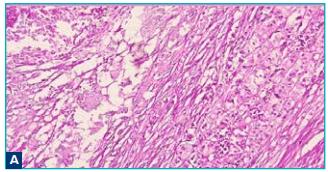
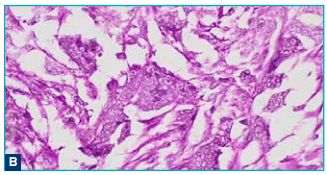
Figure 2: Periodic Acid–Schiff (PAS) stain: A. PAS stain demonstrating intracellular yeast forms of Histoplasma, which appear magenta and are concentrated within histiocytes and areas of necrotic debris (PAS, x20); B. Higher power showing clusters of small budding fungal yeasts with characteristic eccentric nuclei, consistent with Histoplasma capsulatum (PAS, x40).
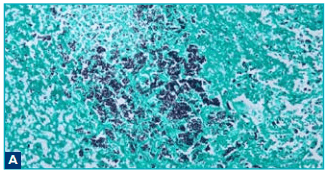
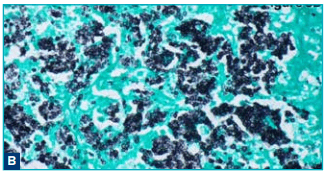
Figure 3: Grocott-Gomori methenamine silver (GMS) stains: A. GMS stain highlighting numerous 2–5 µm Histoplasma yeast forms, which appear as black, round to oval organisms clustered within histiocytes and necrotic tissue (GMS, x20); B. Lower power GMS view showing dense aggregates of fungal organisms distributed within areas of granulomatous inflammation and necrosis (GMS, x40).
Discussion
Adrenal involvement in histoplasmosis is typically associated with progressive disseminated histoplasmosis in immunocompromised hosts, including patients with human immunodeficiency virus (HIV), transplant recipients, or those on long-term corticosteroids.1,2,6 In contrast, isolated adrenal histoplasmosis in an immunocompetent individual, as in this case, is distinctly unusual but increasingly recognised.5,7 The adrenal glands’ rich sinusoidal vasculature and lipidrich cortex create an environment conducive to fungal proliferation. 8,9 While bilateral adrenal involvement often leads to adrenal insufficiency, unilateral disease may remain subtle or entirely asymptomatic.10 In this patient, the infection was discovered incidentally, highlighting the diagnostic challenges posed by atypical presentations. Radiologically, adrenal histoplasmosis can mimic primary adrenal malignancies, metastases, or granulomatous diseases due to heterogeneous enhancement, necrosis, or occasional calcification. 6,10 Hormonal assays are essential to exclude functional adrenal tumours; all results were normal in this case. Histopathology remains the gold standard, with the presence of intracellular budding yeasts serving as the defining diagnostic feature. 10 Management of adrenal histoplasmosis is individualised. Disseminated disease warrants prolonged antifungal therapy, typically itraconazole or amphotericin B, depending on severity. 1,6 In contrast, incidentally detected, localised infections following complete surgical excision may not require additional systemic treatment. Infectious disease consultation is recommended to guide individualised management decisions.
Conclusion:
Isolated adrenal histoplasmosis in immunocompetent individuals is a rare entity that can closely mimic adrenal neoplasms on clinical, biochemical, and radiological evaluation. This case underscores the importance of considering infectious aetiologies, particularly histoplasmosis, in the differential diagnosis of unilateral adrenal masses, even in the absence of systemic symptoms or immunosuppression. Definitive diagnosis relies on histopathological examination with appropriate fungal stains, as imaging and hormonal studies alone may be misleading. Awareness of this uncommon presentation is essential for accurate diagnosis, avoidance of overtreatment, and appropriate postoperative management, including judicious use of antifungal therapy in selected cases.
Aditi Senapati, Anju Shukla, Rahul Yadav. Adrenal Cortical Adenoma with Histoplasmosis in an
Immunocompetent Host – An Incidental Discovery. MMJ. 2026,
March. Vol 3 (1).
References
- Wheat LJ, Azar MM, Bahr NC, et al. Histoplasmosis. Infect Dis Clin North Am. 2016;30(1):207–27.
- Kauffman CA. Histoplasmosis: a clinical and laboratory update.Clin Microbiol Rev. 2007;20(1):115–32.
- Goldblum JR, Lamps LW, McKenney JK. Rosai and Ackerman’s Surgical Pathology. 11th Edition. Elsevier; 2018.
- Weiss S, Goldblum JR, Folpe AL. Enzinger and Weiss’s Soft Tissue Tumors. 7th Edition. Elsevier; 2019.
- Turek D, Graber A, Nienhold R, et al. Pathologie von Infektionskrankheiten [Pathology of infectious diseases]. Ther Umsch. 2019;76(7):391–6.
- Dismukes WE, Pappas PG, Sobel JD. Clinical Mycology. 2nd Edition. Oxford University Press; 2009.
- Pury S, Álvarez MS, Caliva Agüero S, et al. Disseminated histoplasmosis in an immunocompetent pediatric patient. Histoplasmosis diseminada en una paciente pediátrica inmunocompetente.Arch Argent Pediatr.2023;121(3):e202202715.
- Deepe GS Jr. Histoplasma capsulatum. In: Bennett JE, Dolin R, Blaser MJ, editors. Principles and Practice of Infectious Diseases. 9th Edition. Elsevier; 2020. p. 3063–78.
- Lamps LW. Fungal infections. In: Mills and Sternberg’s Diagnostic Surgical Pathology. 7th Edition. Wolters Kluwer; 2022. p. 1625–60.
- Kauffman CA, Pappas PG, Sobel JD, Dismukes WE. Essentials of Clinical Mycology. 2nd Edition. Springer; 2011.