

Abstract:
Gastrointestinal stromal tumours (GISTs) are mesenchymal neoplasms that most commonly arise from the gastrointestinal tract. Prostatic GIST is an extremely rare form of extra-GIST that often presents with obstructive urological and gastrointestinal symptoms. A 39-year-old male presented with acute intestinal obstruction and urinary retention, with a one-month history of intermittent obstructive symptoms. He had been diagnosed with prostatic GIST five years previously and treated with imatinib, which resulted in initial tumour regression. The patient, who had known diabetes mellitus and untreated tuberculosis, developed worsening symptoms and was scheduled for definitive surgical management at Max Super Speciality Hospital, Lucknow. Intraoperatively, a large abdominopelvic mass adherent to the bladder and rectum was excised via a complex multivisceral surgical approach. Histopathology and immunohistochemistry confirmed a malignant GIST. Prostatic GIST is a rare and aggressive tumour that may present with life-threatening obstructive complications. Despite longterm tyrosine kinase inhibitor (TKI) therapy, surgical resection remains essential in cases of progression or acute obstruction.
Key words: Prostatic Gastrointestinal Stromal Tumour, Extra-Gastrointestinal Stromal Tumour (EGIST), Acute Intestinal Obstruction, Acute Urinary Retention, Malignant GIST, Imatinib Therapy.
Introduction
Gastrointestinal stromal tumours (GIST) represent the most common mesenchymal tumours of the gastrointestinal tract and originate from the interstitial cells of Cajal (ICC). The stomach and small intestine are the most frequently involved sites. Extra-gastrointestinal stromal tumours (EGISTs) are rare, accounting for less than 5% of all GISTs, and arise outside the gastrointestinal tract, including the retroperitoneum, mesentery, and pelvis.¹ Prostatic GIST is an exceedingly rare entity that poses significant diagnostic and therapeutic challenges. Due to its location, it often presents with urinary retention, bowel obstruction, or pelvic mass effects, and may be mistaken for more common prostatic malignancies.² The advent of tyrosine kinase inhibitors (TKIs) such as imatinib has revolutionised the management of GIST, however, surgery remains the cornerstone in symptomatic, progressive, or malignant disease.³
Case Report
A 39-year-old male presented with acute intestinal obstruction and acute urinary retention. He reported a one-month history of intermittent abdominal distension, constipation, and difficulty in micturition. The patient had previously undergone a prostatic biopsy at a government tertiary care centre five years earlier, where prostatic GIST was diagnosed. He was started on imatinib therapy, following which the tumour initially regressed. He had known diabetes mellitus and a history of tuberculosis, for which he was not receiving active treatment. On presentation, the patient was catheterised for urinary retention and stabilised. Clinical and radiological evaluation revealed a large pelvic mass causing compression of both urinary and gastrointestinal structures. In view of acute obstruction and disease progression, surgical intervention was planned at Max Super Speciality Hospital, Lucknow, UP.
Intraoperative findings and procedure
A midline abdominal incision revealed a large abdominopelvic mass measuring 15.0 x 13.0 x 9.5 cm, adherent to the urinary bladder and rectum. The urinary bladder was grossly thickened and distended. The mass was abutting the bilateral ureters. There was no ascites or major vascular encasement.
Surgical steps included:
- Initial dissection between the bladder and the mass;the bladder was abutting but not involved, and planes were maintained
- Bilateral ureters were carefully dissected away from the mass up to the bladder base
- Anterior dissection was carried out up to the pubic bone
- Posteriorly, the mass was dissected from the rectum up to its mid-part; however, due to rectal wall adherence, the rectum was divided between the upper and mid-segments
- Further posterior dissection was performed up to the pelvic floor muscles
- The bladder neck was divided to expose the prostate,and the mass was excised
- The urethra was transacted at the bony level and sent for frozen section examination, which showed negative margins
- Bladder neck was anastomosed to the urethra using 4-0 polydioxanone (PDS) double-needle sutures over a Foley catheter
- Suprapubic cystostomy and colostomy were performed
- Drain placement was performed, and the abdomen was closed in layers
The surgery lasted for 8 hours, with an estimated blood loss of approximately 1 L. The postoperative course was uneventful, and the patient was discharged on postoperative Day 7 with regular follow-up.
Histopathological findings
Gross examination revealed a well-encapsulated tumour with areas of necrosis (Figure 1).
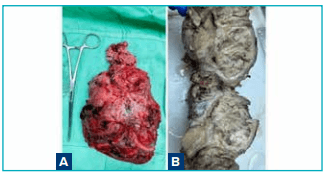
Figure 1: Gross morphology of prostatic gastrointestinal stromal tumour: A. Resected abdominopelvic mass showing a large, lobulated, irregular tumour with congested and haemorrhagic external surface; B. Cut surface of the tumour revealing a solid, grey-white to grey-tan appearance with areas of necrosis.
Microscopic examination showed a highly cellular tumour composed of spindle and epithelioid cells arranged in storiform, fibrosarcomatous, and epithelioid patterns. Extensive areas of hypercellularity, marked cytological atypia, and frequent mitoses, including atypical forms (30–35 per 50 high-power fields), were noted (Figures 2 and 3).
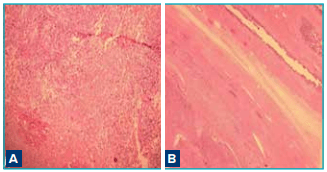
Figure 2: Side-by-side photomicrographs of malignant prostatic gastrointestinal stromal tumour (haematoxylin and eosin [H&E]): A. Tumour showing extensive serpentine areas of necrosis; B. Tumour with adjacent seminal vesicle.
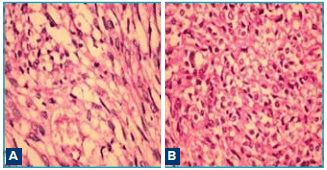
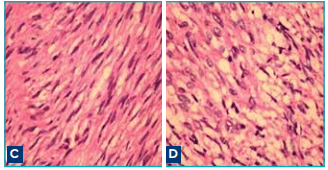
Figure 3: Histopathological features of malignant prostatic gastrointestinal stromal tumour (haematoxylin and eosin [H&E], ×600): A. Tumour showing atypical mitotic figures; B. Epithelioid tumour cell morphology; C. Spindle cell pattern arranged in fascicles; D. High-grade tumour area with marked cellularity and nuclear atypia.
An initial diagnosis of malignant spindle cell tumour was considered. Immunohistochemical evaluation showed(Figure 4):
- CD117 (c-KIT): Positive
- DOG-1: Positive
- CD34: Positive
- SMA: Negative
- S-100: Negative
- Desmin: Negative
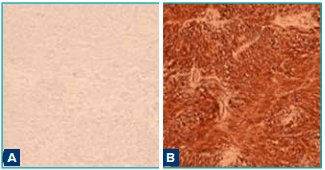
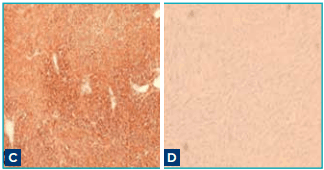
Figure 4: Immunohistochemical profile of prostatic gastrointestinal stromal tumour: A. Desmin: Negative; B. CD-117 (c-KIT): Diffuse strong cytoplasmic and membranous positivity in tumour cells; C. DOG-1: Diffuse strong cytoplasmic positivity confirming gastrointestinal stromal tumour lineage; D. S-100: Negative.
Based on these findings, a final diagnosis of malignant GIST was established.⁴,⁵
Discussion
The cell of origin of GIST is ICC, the pacemaker cell of the gastrointestinal muscles. It is known that ICC expresses the gene product of KIT (CD117), a proto-oncogene that encodes the receptor tyrosine kinase, Kit. Because these ICC cells may exist in diverse anatomic sites, it is possible to explain EGIST of unusual sites such as those of the uterus, vagina, prostate, and bladder.6
Prostatic GIST is an exceptionally rare variant of EGIST, with very few cases reported in the literature. Its presentation is often delayed and dominated by obstructive urinary and bowel symptoms due to its pelvic location.²
The main clinical manifestations of patients with primary EGIST of the prostate include urinary frequency, urgency, dysuria, acute urinary retention, vague perineal pain, and constipation or a combination of one or more of these symptoms. Compared with other GISTs, EGIST masses can grow to a larger volume in the peritoneal cavity and retroperitoneal space, so cases of EGIST are difficult to detect early and need prompt imaging techniques.7
The presented case involved a large mass in the prostate gland, requiring differential diagnosis from other prostatic malignancies such as prostate cancer. However, unlike prostate cancer, which occurs in the elderly, EGISTs can also affect younger patients.
Imatinib is the first-line therapy for unresectable, recurrent, or metastatic GIST and can be used as neoadjuvant or adjuvant therapy.³ While long-term imatinib therapy may lead to tumour regression, resistance or progression can occur, as seen in the presented case. Therefore, radical prostatectomy is the most common form of surgical management. As lymph node metastasis is not common, extensive lymph node dissection is not required.
Malignant features such as high mitotic index, necrosis, cellular atypia, and large tumour size are associated with poor prognosis.8 In such cases, aggressive surgical resection with negative margins remains essential for symptom control and disease management.
The presented case highlights the importance of timely surgical intervention in patients with progressive symptoms despite prolonged targeted therapy, and the need for a multidisciplinary approach in managing rare pelvic GISTs.
Conclusion:
Prostatic GIST is a rare and aggressive tumour that may present with acute intestinal obstruction and urinary retention. Although TKIs play a crucial role in management, surgery remains indispensable in cases of malignant transformation or life-threatening obstructive complications. Early recognition and comprehensive treatment are key to improving outcomes.
Chakradhar Singh, Shashank Chaudhary, Anju Shukla. Malignant Prostatic Gastrointestinal Stromal Tumour Presenting with Acute Intestinal Obstruction and Urinary Retention: A Rare Case Report. MMJ.
2026, March. Vol 3 (1).
References
- Miettinen M, Lasota J. Gastrointestinal stromal tumors:pathology and prognosis at different sites. Semin Diagn Pathol. 2006;23(2):70–83.
- Agaimy A, Wünsch PH, Sobin LH, et al. Extra-gastrointestinal stromal tumors: a clinicopathologic study of 48 cases. Mod Pathol. 2009;22(6):875–84.
- Demetri GD, von Mehren M, Blanke CD, et al. Efficacy and safety of imatinib mesylate in advanced gastrointestinal stromal tumors. N Engl J Med. 2002;347(7):472–80.
- Fletcher CD, Berman JJ, Corless C, et al. Diagnosis of gastrointestinal stromal tumors: a consensus approach. Hum Pathol. 2002;33(5):459–65.
- West RB, Corless CL, Chen X, et al. The novel marker DOG1 is expressed ubiquitously in gastrointestinal stromal tumors.Am J Pathol. 2004;165(1):107–13.
- Huh JS, Park KK, Kim YJ, et al. Diagnosis of a gastrointestinal stromal tumor presenting as a prostatic mass: a case report.World J Mens Health. 2014;32(3):184–8.
- Yang Y, Sun D, Tang K. Primary extragastrointestinal stromal tumors of the prostate: A case report and literature review.Front Oncol. 2022;12:1038853.
- Joensuu H. Risk stratification of patients diagnosed with gastrointestinal stromal tumor. Hum Pathol. 2008;39(10):1411–9.