

Abstract:
Fanconi anaemia (FA) is a rare genetic disorder characterised by bone marrow failure and a high predispositionto malignancy. Haematopoietic stem cell transplantation (HSCT) is the definitive treatment for the haematologicalmanifestations. However, patients with FA exhibit extreme sensitivity to standard conditioning regimens. We present a case of a patient with a confirmed FA complementation group A (FANCA) mutation who developed fatal, rapid-onset acute lung injury (ALI) and acute respiratory distress syndrome (ARDS) approximately three hours after the administration of the first dose of fludarabine as part of a reduced-intensity conditioning (RIC) regimen for an allogeneic HSCT. The patient experienced rapid clinical deterioration, including fever, hypotension, profound hypoxia, and ultimately cardiac arrest, leading to death within 24 hours of drug administration. This case highlights the critical vulnerability of FA patients to severe, precipitous drug toxicity in this high-risk population, although a drug reaction or idiosyncratic reaction seems most likely..
Key words: Fanconi Anaemia, Fludarabine, Acute Lung Injury, Acute Respiratory Distress Syndrome,Haematopoietic Stem Cell Transplantation, Drug Toxicity.
Introduction
Fanconi anaemia (FA) is an autosomal recessive or X-linked disorder caused by mutations in genes responsible for deoxyribonucleic acid (DNA) repair. This condition leads to progressive bone marrow failure, congenital anomalies, and an increased risk of cancer. Allogeneic haematopoietic stem cell transplantation (HSCT) remains the primary curative treatment for the haematological complications of FA. However, the use of conventional myeloablative conditioning regimens has historically resulted in high rates of toxicity and mortality due to the underlying cellular hypersensitivity of FA patients to DNA-damaging agents.1,2 Reducedintensity conditioning (RIC) regimens utilising agentslike fludarabine have improved outcomes, but toxicity concerns persist. Fludarabine-induced pulmonary toxicity is a recognised adverse event, typically manifesting as a later-onset interstitial pneumonitis or acute respiratory distress syndrome (ARDS) with a median onset of 21 days.3 We report an exceptionally rare case of immediate, fata ARDS onset within hours of initial fludarabine exposure in a patient with FA, underscoring a unique and heightened susceptibility to this agent.
Case Report
A patient diagnosed with FA, confirmed by the identification of a pathogenic FA complementation group A (FANCA) mutation and presenting with severe pancytopenia, was admitted to the Department of Haematology-Oncology and Bone Marrow Transplantation for a planned allogeneic HSCT. The donor was a fully human leukocyte antigen (HLA)-matched sibling. A standard RIC regimen, which included fludarabine, was initiated. Figure 1 shows the initial chest X-ray (CXR) taken after insertion of the peripherally inserted central catheter (PICC) line.
Approximately three hours following the administration of the initial dose of fludarabine, the patient experienced abrupt and rapid clinical deterioration. This acute event was characterised by the onset of recurrent high-grade fever, systemic hypotension, and profound hypoxia that necessitated immediate high-flow oxygen support and escalation of care. A CXR was performed, which revealed widespread bilateral diffuse haziness consistent with ARDS (Figure 2), whereas the CXR prior to fludarabine administration was normal (Figure 1). Despite aggressive resuscitation efforts and intensive supportive care, the patient's condition rapidly progressed to irreversible respiratory failure. The patient expired within 24 hours of receiving the initial fludarabine dose.
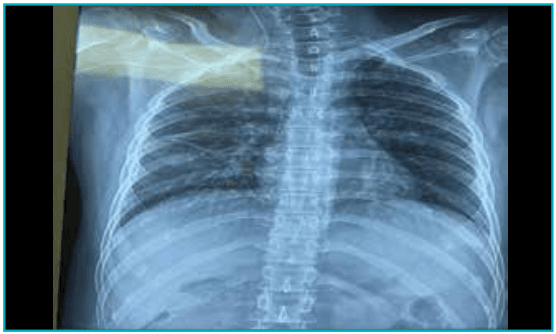
Figure 1: Showing a normal chest X-ray.
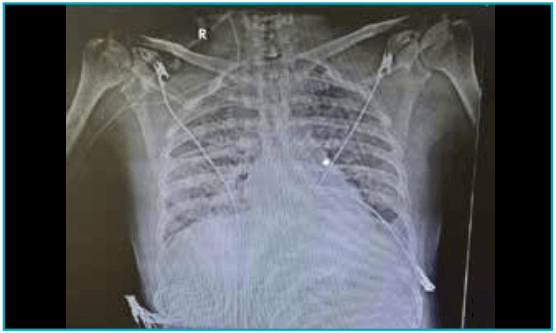
Figure 2:Showing bilateral infiltrates developed after four hours of 1stchest X-ray.
Discussion
This case highlights the extreme and immediate vulnerability of patients with FA to the severe toxicities of conditioning agents, even those typically considered less myeloablative or associated with later-onset toxicities.Fludarabine pulmonary toxicity is a known, albeit generally uncommon, adverse event following HSCT, usually developing one to two weeks after the final course of chemotherapy or a median of 21 days post-transplant. 3,4 The temporal association of drug administration and the development of acute respiratory failure in a patient with normal lungs points towards a drug-induced idiosyncratic reaction. The underlying genetic defect in DNA repair widespread bilateral diffuse haziness consistent with ARDS (Figure 2), whereas the CXR prior to fludarabine administration was normal (Figure 1). Despite aggressive resuscitation efforts and intensive supportive care, the patient's condition rapidly progressed to irreversible respiratory failure. The patient expired within 24 hours of receiving the initial fludarabine dose.mechanisms specific to FA as a likely predisposing factor cannot be excluded.This critical outcome underscores a vital clinical necessity:the implementation of hyper-vigilant monitoring protocols for FA patients during the administration of all conditioning agents. At the earliest sign of pulmonary compromise,fever, or any Worsening clinical status due to infection,immediate cessation of potentially causative agents must be considered. This case serves as a stark reminder of the unique high-risk profile of the FA patient group, where standard drug kinetics and toxicity profiles may not apply.
Conclusion:
Fludarabine can induce a rare, rapid-onset fatal acute lung injury (ALI) in patients with FA receiving HSCT conditioning. Clinicians must maintain a high index of suspicion for atypical and severe toxicities in this population and employ highly cautious and individualised treatment protocols.
Anamika Bakliwal, Sanjeev Kumar Sharma. Within Hours: A Catastrophic Reaction to Fludarabine in Fanconi
Anaemia. MMJ. 2026, March. Vol 3 (1).
References
- Deeg HJ, Auerbach AD. Allogeneic bone marrow transplantation in Fanconi anemia. A survey of the International Bone Marrow Transplant Registry. Blood. 1990;76(8):1642–48.
- Gluckman E, Auerbach AD, Bacigalupo A, et al. Bone marrow transplantation for Fanconi anemia: an international cooperative study. Br J Haematol. 2011;155(5):585–93.
- Helman DL Jr, Byrd JC, Ales NC, et al. Fludarabine-related pulmonary toxicity: a distinct clinical entity in chronic lymphoproliferative syndromes. Chest. 2002;122(3):785–90.
- Lee SJ, Deeg HJ, Storer B, et al. Fludarabine-based conditioning for patients with severe aplastic anemia or myelodysplastic syndrome undergoing hematopoietic cell transplantation. Br J Haematol. 2006;134(3):329–33.