

Abstract:
Unilateral absence of pulmonary artery (UAPA) is an uncommon condition with a prevalence of 1 in 200,000 young adults, which is characterised by congenital absence of either the left or right pulmonary artery and may be associated with or without other cardiac diseases. While the UAPA declares itself in infancy when associated with other congenital anomalies, patients with isolated UAPA usually remain asymptomatic and present in adulthood with symptoms such as dyspnoea, haemoptysis, recurrent infections, etc. We encountered an adult male patient who presented with haemoptysis and was diagnosed on further examination to have an absent right pulmonary artery. Considering the rarity and non-specific presentation of isolated UAPA, this case is being reported.
Key words: Unilateral Absence of Pulmonary Artery, Haemoptysis, Congenital Cardiac Anomaly.
Introduction
Unilateral pulmonary artery agenesis is a rare congenital abnormality characterised by the congenital absence of either the left or right pulmonary artery due to failure of the sixth ipsilateral aortic arch during embryogenesis.1 Most commonly, unilateral absence of pulmonary artery (UAPA) occurs in conjunction with cardiovascular abnormalities such as right aortic arch, patent ductus arteriosus, tetralogy of Fallot, or cardiac septal defects, but rarely, it can present in an isolated manner.2,3 Isolated UAPA (IUAPA) involves the right lung in about two-thirds of cases.4 Due to embryologic relationships, UAPA commonly occurs on the side of the chest opposite the aortic arch.5 In adults, it is often detected incidentally on chest computed tomography (CT) imaging performed for other indications. There is limited knowledge on the incidence, presentation, and management of IUAPA. We report such a case in an adult with non-specific symptoms.2-4
Case Report
A 36-year-old male presented with a history of recurrent haemoptysis since three days. There was no fever, cough, expectoration, chest pain, breathlessness, palpitation or syncope. Family history was negative for any congenital heart disease. There was a past medical history of preterm birth, and the patient underwent left cheiloplasty in childhood (no documents available at present). The patient denied any history of smoking, alcohol or drug abuse.
Physical examination revealed a fairly built male adult. Vitals were within normal limits. There was no clubbing, cyanosis, hepatomegaly, or pedal oedema. Jugular venous pressure was not raised. Respiratory and cardiovascular examinations were normal, except for a medial shift of the apex beat to the fifth intercostal space, just lateral to the left sternal border.
Electrocardiogram, two-dimensional echocardiography, and resting arterial blood gas analysis were within normal limits. Spirometry was not performed in view of active haemoptysis. Chest X-ray posteroanterior view (Figure 1) showed reduced right lung volume with ipsilateral shift of mediastinum.
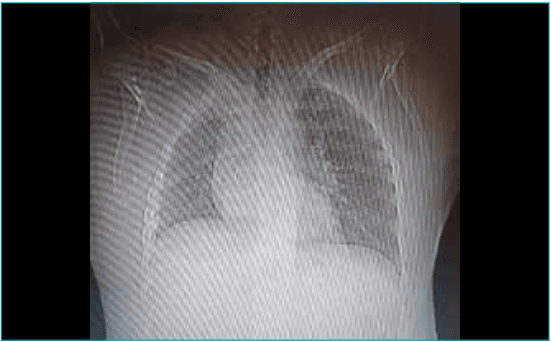
Figure 1: Chest X-ray posteroanterior view showing a small right hemithorax with shift of the mediastinum towards the right side.
CT pulmonary angiography (Figures 2–4) showed proximal interruption of the right pulmonary artery with narrowed right pulmonary veins and multiple systemic collaterals supplying the right hilum. There were ipsilateral right-sided pulmonary hypoplasia, reticulations, small cysts in the right basal segments, and serrated pleural thickening, with hyperinflated left lung and hypertrophied left pulmonary artery and veins.
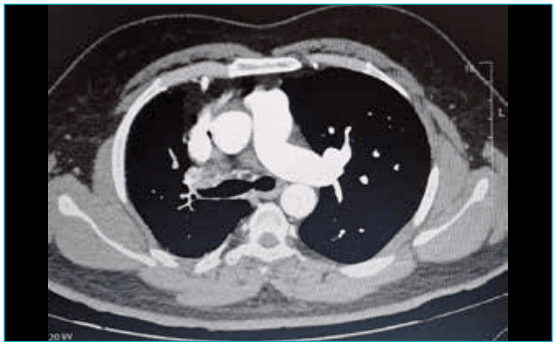
Figure 2: Computed tomography pulmonary angiography showing proximal interruption of the right pulmonary artery and hypertrophied left pulmonary artery and veins.
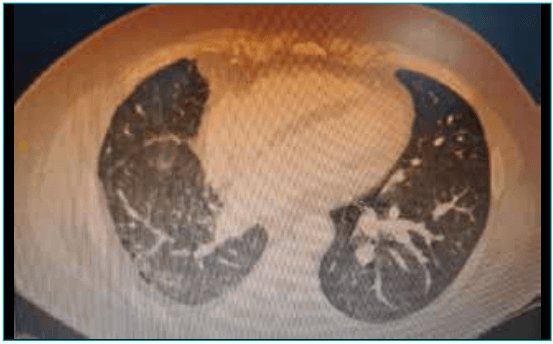
Figure 3: Ipsilateral right-sided pulmonary hypoplasia, reticulations, small cysts in the right basal segments, and serrated pleural thickening with hyperinflated left lung.
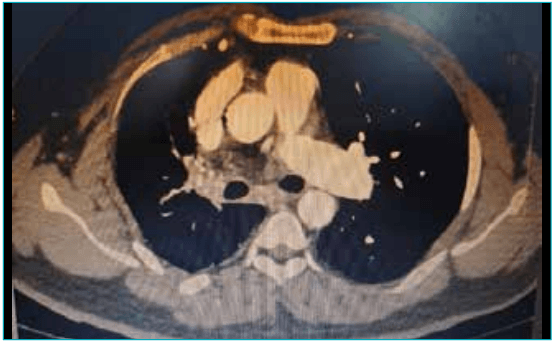
Figure 4: Narrowed right pulmonary veins and multiple systemic collaterals supplying the right hilum.
A diagnosis of absent right pulmonary artery was made, and symptomatic treatment was given to the patient. Haemoptysis subsided within the next 24 hours.
Discussion
Embryologically, pulmonary vasculature develops from three principal sources. The main pulmonary artery is derived from the arterial portion of the truncus arteriosus. The extrapulmonary portion of pulmonary arteries develops from the respective sixth branchial arch, while the intrapulmonary vasculature develops from their respective mesenchymal tissue surrounding the lung buds. Agenesis of pulmonary artery is due to the involution of sixth branchial arch. Since the intrapulmonary vasculature, which develops from the respiratory mesenchyme, is normal in these patients, the lung receives blood retrogradely from collateral arteries and from a persistent ductus arteriosus.6 “Interruption” is a term that has also been used by several authors for this condition.7 Earlier, the term "absence of pulmonary artery" was widely used for this condition. However, recent consensus in the scientific literature states that as the intrapulmonary vascular network is still intact, the term “interruption of the pulmonary artery” is preferred over “absence of pulmonary artery”.8 Common collaterals supplying the lung include bronchial arteries, transpleural branches of intercostals, internal mammary, subclavian, and innominate arteries.9 Rarely, collaterals from the coronary arteries also supply the lung with an absent pulmonary artery.4 Most commonly, UAPA occurs in conjunction with cardiovascular abnormalities such as tetralogy of Fallot or cardiac septal defects, but it can also occur in an isolated manner.2,3 Isolated UAPA involves the right lung in about two thirds of cases.4 Due to embryologic relationships, UAPA commonly occurs on the side of the chest opposite the aortic arch.5 During the first half of the 20thcentury, all recorded cases of absent pulmonary artery were from the autopsy series.4
Subsequently, with the availability of cardiac surgery in the early seventies for cyanotic heart diseases, many more cases were identified at the time of surgery.3,10After the development of angiographic techniques, diagnosis of this entity was possible without surgery or autopsy.11 The advent of CT in the last quarter of the 20thcentury made the diagnosis of this entity even easier. Patients were diagnosed with this abnormality when CT was performed for the evaluation of other unrelated chest problems or during the work-up of symptoms related to this abnormality, e.g. haemoptysis and dyspnoea.7,8
Occasionally, these cases can also be diagnosed when a chest X-ray is performed as part of a routine check-up or during a pre-employment examination. A small hemithorax with diffuse reticulations due to collateral blood supply from the systemic circulation to the lung points towards the possibility of an absent pulmonary artery and the need for further work-up.4,8 However, a smaller hemithorax may also be seen in scimitar syndrome and hypoplastic lung. Congenital hypoplastic lung and absent or hypoplastic pulmonary artery disease can be excluded from scimitar syndrome by the presence of normal venous drainage to the left atrium.3,8
On CT scan, the affected part of the pulmonary artery terminates within 1 cm of its origin. Direct anastomosis of transpleural collateral vessels with peripheral branches of the pulmonary artery appears as serrated thickening of the pleura and subpleural parenchymal bands on CT film. Such a CT appearance may mimic interlobular septal thickening as seen in idiopathic pulmonary fibrosis (IPF).10 Contrast-enhanced CT of the chest not only diagnoses an absent pulmonary artery but also provides information about mediastinal structures and lung parenchyma. As per Shostak E et al, invasive angiography is better in certain aspects as it provides better delineation and haemodynamic data; however, pulmonary angiography should be reserved only for those having structural cardiac anomalies on echocardiography.12
A subject with an IUAPA may experience recurrent respiratory infections, dyspnoea on exertion, high-altitude pulmonary oedema, pulmonary hypertension in the contralateral lung or haemoptysis.13 Haemoptysis occurs in about 20% of cases and is usually self-limiting. Occasional case reports of massive haemoptysis and death are available in the literature.4 Rupture of an aneurysm between systemic to pulmonary collateral is said to be responsible for haemoptysis.
There is no consensus regarding treatment of this condition. However, those who are asymptomatic or have minor symptoms should be observed closely for the development of pulmonary arterial hypertension. Medical treatment of pulmonary hypertension in patients with UAPA without associated congenital heart disease is not yet available.12 Surgical options to correct pulmonary hypertension, when present, include anastomosis of the hilar arteries of the affected lung to the main pulmonary artery.12 Pneumonectomy is to be considered in cases with massive haemoptysis.14 In patients with poor pulmonary reserve and/or comorbid conditions, selective embolisation of the systemic artery is indicated for the management of haemoptysis.13
Conclusion:
IUAPA is a rare congenital anomaly that may remain clinically silent until adulthood and is often detected incidentally on imaging performed for unrelated indications. Awareness of its characteristic radiological features is essential to avoid misdiagnosis and to distinguish it from other causes of a small hemithorax such as scimitar syndrome or pulmonary hypoplasia. CT pulmonary angiography plays a pivotal role in diagnosis by accurately delineating vascular anatomy, systemic collaterals, and associated parenchymal changes. Management remains individualised, with close follow-up required to monitor for complications such as pulmonary hypertension and haemoptysis.
Nikhil Tomar, Taha Nabeel, Pritha Nayyar, Ashish Jain. Isolated Unilateral Absence of Pulmonary Artery in
an Adult. MMJ. 2026, March. Vol 3 (1).
References
- Sperry Bailey, Thomas Marston. Unilateral pulmonary artery agenesis: The initial diagnosis and adult presentation with massive hemoptysis. Chest. 2024;166(4):A5946–7.
- Bouros D, Pare P, Panagou P, et al. The varied manifestations of pulmonary artery agenesis in adulthood. Chest. 1995;108:670–6.
- Presbitero P, Bull C, Haworth SG, et al. Absent or occult pulmonary artery. Heart. 1984;52(2):178–85.
- Ten Harkel AD, Blom NA, Ottenkamp J. Isolated unilateral absence of a pulmonary artery: a case report and review of the literature. Chest. 2002;122(4):1471–7.
- Pfefferkorn JR, Löser H, Pech G, et al. Absent pulmonary artery. A hint to its embryogenesis. Pediatr Cardiol. 1982;3(4):283–6.
- Sotiria CA, Nikolaos LK, Elias NB, et al. Absent pulmonary artery in one adult and five pediatric patients: imaging, embryology and therapeutic implication. AJR Am J Roentgenol. 2002;179:1253–60.
- Morgan PW, Foley DW, Erickson SJ: Proximal interruption of a main pulmonary artery with transpleural collateral vessels: CT and MR appearances. J Comput Assist Tomogr. 1991.15:311–3.
- Castañer E, Gallardo X, Rimola J, et al. Congenital and acquired pulmonary artery anomalies in the adult: radiologic overview. Radiographics. 2006;26:349–7
- Gupta K, Livesay JJ, Lufschanowski R. Absent right pulmonary artery with coronary collaterals supplying the affected lung. Circulation. 2001;104(4):e12–3.
- Sotomora RF, Edwards JE. Anatomic identification of so-called absent pulmonary artery. Circulation. 1978;57(3):624–33.
- Moreno-Cabral RJ, McNamara JJ, Reddy VJ, et al. Unilateral absent pulmonary artery: surgical repair with a new technique. J Thorac Cardiovasc Surg. 1991;102(3):463–5.
- Shostak E, Sarwar A. A 50-year-old woman with dyspnea, lower extremity edema, and volume loss of the right hemithorax. Chest. 2009;136(2):628–32.
- Yoon W, Kim FK, Kim YH, et al. Bronchial and non-bronchial systemic artery embolizaion for life- threatening hemoptysis: a comprehensive review. Radiographics. 2002;22:1395–409.
- Hentrich F, Stoermer J, Wiesemann G. Unilateral proximal aplasia of the pulmonary artery--studies on the clinical significance and embryologic interpretation. Klinische Padiatrie. 1984;196(5):311–4.