

Abstract:
Hereditary haemorrhagic telangiectasia (HHT), also referred to as Osler-Weber-Rendu syndrome, is a rare autosomal dominant disorder characterised by abnormal vasculogenesis affecting the skin, mucosal surfaces, and visceral organs. Radiological imaging — particularly ultrasound, triple-phase contrast-enhanced computed tomography (CECT), and magnetic resonance imaging (MRI) — serves as a crucial tool for the evaluation of hepatic involvement in these patients. This case report discusses a 74-year-old male who presented to the outpatient department with abdominal pain. The report provides an overview of the characteristic imaging findings of hepatic HHT and discusses the relevant clinical symptomatology and therapeutic strategies.
Key words: Hereditary Haemorrhagic Telangiectasia, Osler-Weber-Rendu Syndrome, Triple-Phase ContrastEnhanced Computed Tomography, Magnetic Resonance Imaging.
Introduction
Hereditary haemorrhagic telangiectasia (HHT) is a rare autosomal dominant genetic disorder. It is also known as Osler-Weber-Rendu syndrome. It causes abnormal development of blood vessels in areas like the skin, mucous membranes, and internal organs, including the lungs, liver, and brain. This condition is caused by mutations in the activin A receptor type II-like 1 (ACVRL1), endoglin (ENG), or SMAD family member 4 (SMAD4) genes, all of which play a role in blood vessel formation.
Diagnosis is based on internationally recognised Curaçao (or consensus) criteria,1 which focus on four key features:
(i) Recurrent spontaneous nosebleeds (epistaxis)
(ii) A family history of HHT
(iii) Mucocutaneous telangiectasias
(iv) Involvement of internal organs
Based on the number of criteria present, the diagnosis is classified as definite (three or more criteria), possible/ suspected (two criteria), or unlikely (one or none). 2
Among the organs affected by HHT, the liver is most frequently involved. 3 Approximately one-third of patients develop hepatic arteriovenous malformations, which are a growing clinical concern. 1 Liver involvement can vary widely — from small telangiectasias to larger, confluent vascular lesions. In most cases, these malformations do not cause symptoms, with fewer than 10% of patients experiencing related clinical signs. 4
When present, symptoms typically depend on the dominant type of hepatic vascular shunting: arteriovenous, arterioportal, or portovenous. 5 Imaging studies, such as ultrasound, computed tomography (CT) scans, and magnetic resonance imaging (MRI), are vital for assessing liver complications. 2 However, multiphasic CT is considered the most effective noninvasive method for diagnosing hepatic involvement in HHT and identifying the specific types of shunts. 5
Clinical manifestations vary according to the type and extent of vascular shunting: arteriosystemic (arteriovenous) shunts can result in high-output cardiac failure (HOCF); arterioportal shunting may lead to portal hypertension, 2 whereas portovenous shunts can cause hepatic encephalopathy. In addition, diversion of blood from the mesenteric circulation through the hepatic artery may lead to mesenteric ischaemia. 5
Case Report
A 74-year-old male patient presented to the outpatient department with complaints of abdominal pain. An ultrasound examination done earlier revealed mild intrahepatic bile duct dilatation, with no other significant abnormalities. Subsequently, the patient was advised to undergo triple-phase CT of the abdomen, which revealed findings consistent with HHT
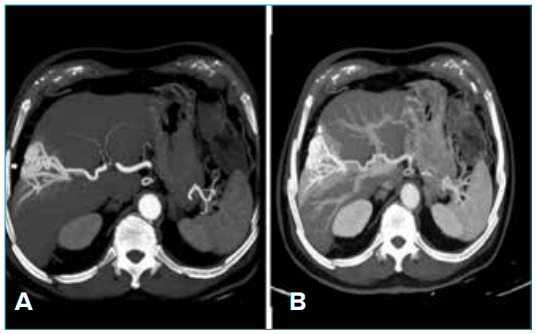
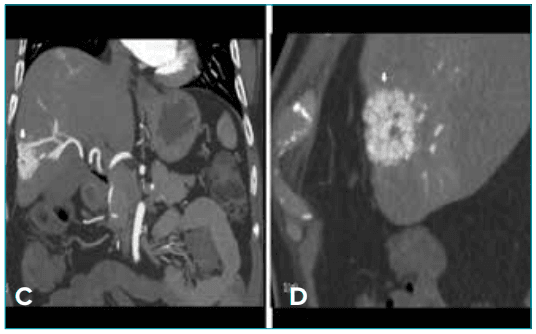
Figure 1: A, B. Axial; C. Coronal; and D. Sagittal triple-phase computed tomography (CT) images in the arterial phase showing a dilated hepatic artery and multiple telangiectatic vessels (arrow), along with hepatic arterioportal shunting, marked by early opacification of the portal vein.
Radiological findings
Triple phase CT abdomen revealed a dilated hepatic artery and multiple telangiectatic vessels along with hepatic arterioportal shunting marked by early opacification of portal vein during arterial phase (Figure 1A–D). Two foci of hyper vascular lesions with hepatic arterioportal shunting were seen during portal phase (Figure 2A–C). Multiple telangiectatic vessels were seen during delayed phase (Figure 3A and B). Three-dimensional (3D)-reconstructed coronal images revealed a dilated hepatic artery and vascular telangiectasia (Figure 4A and B).
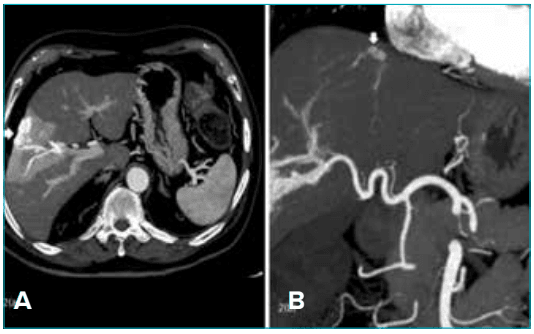
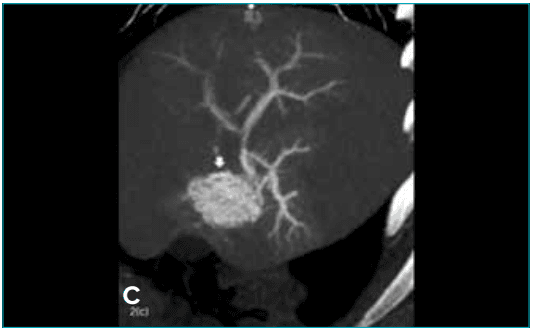
Figure 2: A, Axial; B. Coronal; C. Sagittal triple-phase computed tomography (CT) images during portal phase showing two foci of hyper vascular lesions (arrow) with hepatic arterioportal shunting
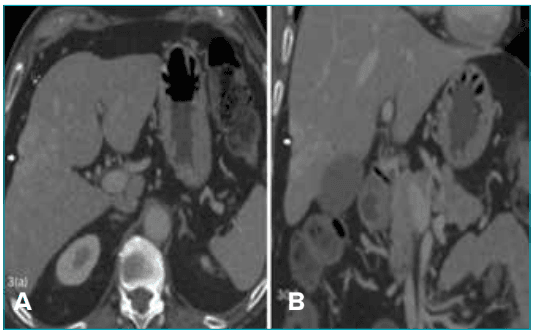
Figure 3: A, Axial; B. Coronal triple-phase computed tomography (CT) images during the delayed phase showing multiple telangiectatic vessels (arrow).
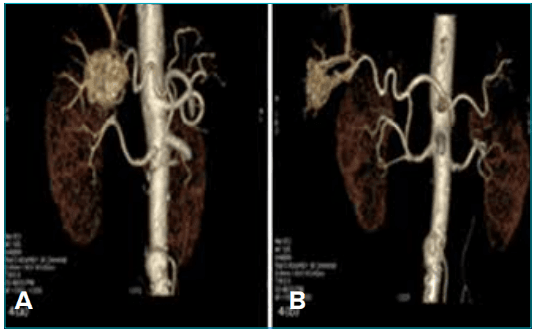
Figure 4: A, B. Three-dimensional (3D) reconstructed coronal images showing a dilated hepatic artery and vascular telangiectasias.
Discussion
In HHT, liver involvement typically features widespread intrahepatic vascular malformations that result in blood flow shunting — including arteriovenous, arterioportal, and/or portovenous pathways. In more than two-thirds of cases, the type of shunt can be identified on imaging by observing early or selective contrast enhancement of the hepatic veins (suggesting arteriovenous shunting) or the portal veins (indicating arterioportal shunting) during different imaging phases. These hepatic changes may appear either as diffuse telangiectasias scattered throughout the liver or as distinct arteriovenous malformations
Although the relationship between specific gene mutations and clinical presentation is still being studied, hepatic involvement is most commonly associated with activin receptor-like kinase 1 (ALK1) gene mutations and is rare in patients with ENG mutations. 6 Typical imaging findings in HHT-related liver disease include dilated, tortuous branches of the hepatic artery, along with premature filling of the portal vein (Figure 1A–D ), heterogenous hepatic parenchymal enhancement during the arterial phase, and multiple hepatic nodules. In the present case, a triple-phase contrast-enhanced CT (CECT) scan was performed, which showed normal contrast uptake in the main portal vein and all three hepatic veins. However, arterial phase opacification of the peripheral portal vein branches was observed, consistent with arterioportal shunting (Figure 1 A–D). 4
Treatment of hepatic vascular malformations is symptom-driven. In patients with arteriovenous shunts causing HOCF, management includes diuretics, salt restriction, and anti-angiogenic medications. In cases of arterioportal shunting leading to portal hypertension, treatment options include fluid restriction and betablockers. 2 Despite these management strategies, liver transplantation remains the only curative treatment for hepatic involvement in HHT. 6 However, asymptomatic individuals with hepatic vascular malformations typically do not require treatment, as most remain free of complications. 2
Conclusion:
This case report describes the characteristic imaging findings of hepatic involvement in HHT, emphasising the importance of recognising different vascular shunts and arteriovenous malformations, which directly influence clinical manifestations and guide patient management. Further imaging evaluation is required to assess pulmonary and cerebral involvement.
Prem Kumar Ganesan, Arindam Mukherjee, Sejal Kanwar. Hepatic Hereditary Haemorrhagic Telangiectasia: A Case report. MMJ. 2026, March. Vol 3 (1).
2026, March. Vol 3 (1).
References
- Khan AR, Waqar S, Wazir MH, et al. A rare case of hereditary hemorrhagic telangiectasia: a case report. Cureus. 2022;14(4).
- Harwin J, Sugi MD, Hetts SW, et al. The role of liver imaging in hereditary hemorrhagic telangiectasia. J Clin Med. 2020;9(11):3750.
- Song W, Zhao D, Li H, et al. Liver findings in patients with hereditary hemorrhagic telangiectasia. Iran J Radiol. 2016;13(4):e31116.
- Jiang J, Wang X, Yang D, et al. Liver involvement in a hereditary hemorrhagic telangiectasia patient with Gd-EOB-DTPA enhanced MRI: a case description. Quant Imaging Med Surg. 2022;12(9):4691.
- Wu JS, Saluja S, Garcia-Tsao G, et al. Liver involvement in hereditary hemorrhagic telangiectasia: CT and clinical findings do not correlate in symptomatic patients. Am J Roentgenol. 2006;187(4):W399–405.
- Garcia-Tsao G. Liver involvement in hereditary hemorrhagic telangiectasia. J Hepatol. 2007;46(3):499–507.