

Abstract:
In this paper, we present our experience regarding the surgical management of asymptomatic renal calculi in the setting of living donor renal transplantation using ex-vivo uretero-renoscopy (URS) following bench preparation, as well as the long-term outcomes of recipients of such kidneys. Between January 2015 and November 2022, 273 possible donors were evaluated at our centre, of whom 15 were found to have urolithiasis during assessment, of whom 7 were accepted for donation. We employed semi-rigid URS during bench surgery for stone removal. Out of the 7 live-related renal allograft transplants studied, all recipients were male, whereas 5 donors were female and 2 were male. The median donor age was 48 years, while the median recipient age was 43.5 years. The most common location for the calculi was the lower calyx, and the median stone size was 5.35 mm. The median cold ischaemia time during surgery was 33.57 minutes. The recipients were found to have adequate graft function, without any stone recurrences after a median follow-up period of 2 years, suggesting that ex-vivo semi-rigid URS is a reasonable option for managing urolithiasis in the graft kidney in selected cases.
Key words: Kidney Transplant, Living Donor, Urolithiasis, Semi-Rigid Uretero-Renoscopy (URS), Bench Surgery.
Introduction
It has been widely accepted that pre-emptive living donor transplantation before dialysis is optimal and is associated with the best outcomes in patients with chronic kidney disease.1,2 The shortage of organs for transplantation has necessitated the implementation of different strategies, such as donation after cardiac death and acceptance of extended criteria donors.
Among the relative contraindications for renal donation, nephrolithiasis has increased in incidence over recent years.3 The danger posed by stone-related complications to an immunosuppressed recipient is significant. Given the urgent need to increase the number of available renal allografts, several studies have explored the feasibility of using kidney grafts with urolithiasis. Multiple centres have reported acceptable outcomes as well.4
The Amsterdam Forum on the Care of the Live Kidney Donor outlines certain criteria for accepting a prospective donor with a history of a solitary stone, as follows:
(a) no hypercalciuria, hyperuricaemia, or metabolic acidosis
(b) no hyperoxaluria or cystinuria
(c) no urinary tract infection
(d) no evidence of multiple calculi or nephrocalcinosis on computed tomography (CT) scan5
Thus, with the ever-increasing need for more donors, nephrolithiasis no longer precludes renal donation.
Here we present our surgical experience with ex-vivo stone removal from renal allografts of living kidney donors using semirigid uretero-renoscopy (URS) after bench dissection, as well as the long-term follow-up of the recipients of these allografts.
Materials and Methods
Our retrospective study included 273 potential donors, among whom 15 were diagnosed with urolithiasis during pre-transplant evaluation. Seven of these donors were accepted, all of whom had asymptomatic renal calculi, along with normal metabolic workup for stone disease. All donor-recipient pairs were informed of the risks associated with bench surgery, and informed consent was obtained.
Following laparoscopic donor nephrectomy, cold perfusion, and bench dissection, with the kidney placed in an ice slush, the distal ureter was held between forceps by two assistants. Next, a 4.5/6.5 Fr semi-rigid uretero-renoscope (Richard Wolf) was introduced into the ureter with cold normal saline irrigation. A pathfinder was used sparingly in case of obscure vision. With the kidney kept fixed by another assistant, the uretero-renoscope could be negotiated into all renal calyces. Calculi were removed using an NGage nitinol stone extractor (Cook Medical). In the event that the target calyx could not be accessed, the team had prepared for endoscopy via a pyelotomy incision as well (Figure 1 and Figure 2).

Figure 1: Ex-vivo uretero-renoscopy being attempted using a semi-rigid uretero-renoscope.

Figure 2: Handling of the ureter by the endoscopist using ring-tipped forceps.
After removal of all calculi, the kidney was placed in the recipient via the open technique. Ureteroneocystostomy was done using the Lich-Gregoir technique, over a 6 Fr, 16 cm long double-J (DJ) stent (Aster Medispro). The DJ stent was removed after 10-14 days.
In addition to the demographic data of the donors and recipients, stone size, stone density in Hounsfield units (HU), stone location, duration of bench surgery, warm ischaemia time, and cold ischaemia time were documented. Postoperative complications were assessed as per the Modified Clavien-Dindo Classification. Long-term follow-up of the recipients included monitoring of serum creatinine levels and the incidence of stone recurrence.
Results
A total of seven living donor renal transplants were studied. Five of the donors were spouses of the recipients. The median age of the donors was 48 years (interquartile range [IQR] 39-60 years) and that of the recipients was 43.5 years (IQR 23-56 years).
None of the donors had any symptoms pertaining to urolithiasis. One donor had previously undergone left URS for a lower ureteric calculus, three years before the kidney donation workup. In all cases, renal calculi were diagnosed either on ultrasound (USG) or on CT angiography during workup.
The average stone size was 5.35 mm (IQR 4.5-6.5 mm). The average stone density was 843 HU (IQR 450-1100 HU). In four donors, the calculus was located in the lower calyx (57.1%). Metabolic evaluation was normal in all donors. Three donors had calculi of ≥6 mm size (6.0 mm, 6.0 mm and 6.5 mm), for whom preparations for pyelotomy and/or laser lithotripsy were in place at the time of bench surgery. However, these stones were successfully extracted using the NGageTM basket. Stone analysis revealed that four calculi were composed of calcium oxalate monohydrate, while three were urate calculi. Table 1 summarises demographics of donors and stone characteristics.
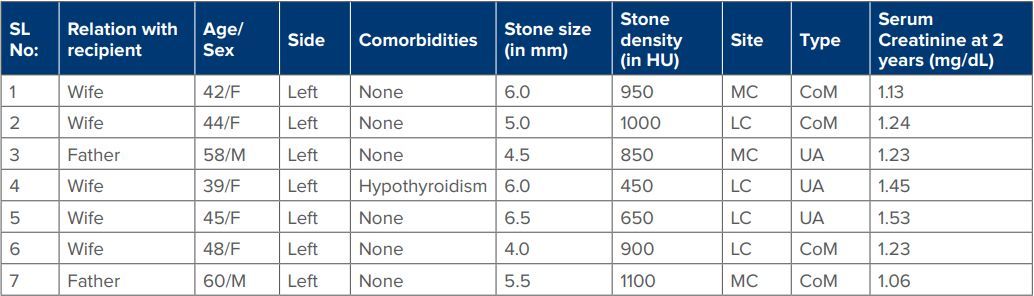
Table 1: Demographics of donors and stone characteristics.
Abbreviations: F: female; M: male; mm: millimetres; HU: Hounsfield units; MC: mid-calyx; LC: lower calyx; CoM: calcium oxalate monohydrate; UA: uric acid.
The median cold ischaemia time was 33.57 minutes (IQR 28- 37 minutes). The median time taken for stone removal was 10.86 minutes (IQR 8-12.5 minutes). One recipient developed postoperative paralytic ileus, which was managed conservatively.
At the 24-month follow-up, all renal allografts were functioning well, with one recipient displaying elevated serum creatinine levels (1.75 mg/dL). No recipients experienced stone-related adverse events. Table 2 summarises demographics of recipient population and outcomes.
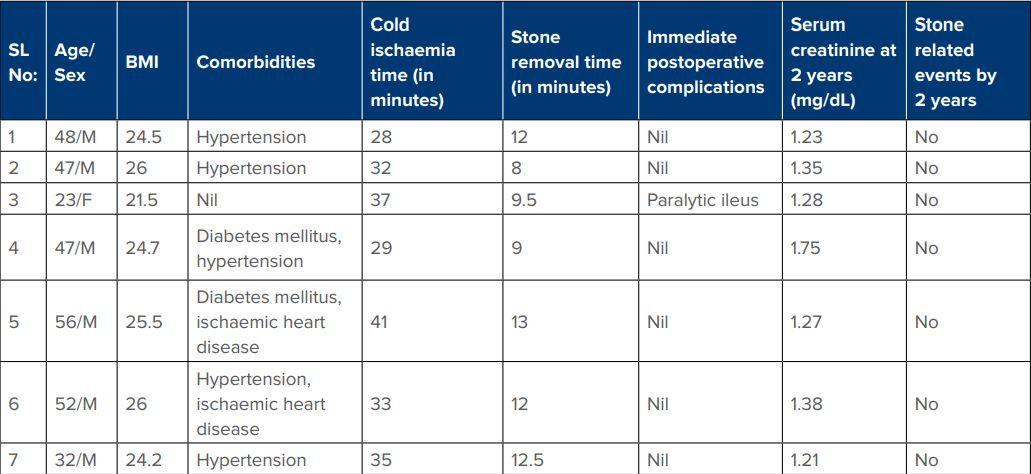
Table 2: Demographics of recipient population and outcomes
Abbreviations: M: male; F: female; BMI: body mass index.
Discussion
Urolithiasis is one of the most common metabolic disorders worldwide. The incidence of renal stone disease in Asians is 1%-5%.6 Urolithiasis was previously considered a relative contraindication to kidney donation. However, at present, it can be managed before, during, or after renal transplantation.
Symptoms of stone disease in a recipient may be atypical, due to graft denervation at the time of donor nephrectomy. Patients may present with elevated serum creatinine levels, oliguria or anuria, and signs of sepsis, without experiencing pain.7 Additionally, management of such cases is significantly challenging, with a possible need for percutaneous interventions.8 Hence, it is preferable to remove calculi from the donor kidney either prior to donor nephrectomy or through ex-vivo bench surgery after nephrectomy. This approach allows to expand the donor pool at a time when scarcity of renal allografts forces more patients towards indefinite dialysis and its associated impact on quality of life.
In such cases, pre-transplant management options include extracorporeal shockwave lithotripsy (ESWL) and retrograde intra-renal surgery (RIRS). The primary concerns associated with ESWL include the risk of residual stone fragments, which are also associated with higher stone recurrence rates, as well as the risk of renal trauma and subsequent renal dysfunction.9,10
RIRS has been linked to complications such as ureteric strictures, renal trauma, and subcapsular collections, which may contribute to renal dysfunction. In addition to the increased costs associated with pre-transplant interventions and the risk of procedure-related complications, delaying transplantation must be considered. Given these factors, we believe that exvivo stone retrieval after donor nephrectomy is a viable option in selected cases.
In our series, none of the recipients who received kidneys that underwent ex-vivo URS experienced stone recurrence. Despite longer cold ischaemia times, there was no cases of delayed graft function. A larger series by Jan et al. with 57 donor-recipient pairs with a median follow up of 3.5 years reported no stonerelated adverse events in any of the recipients.11 Another study by Pushkar et al. involving 14 cases with stone sizes ranging from 4 to 10 mm, reported that smaller calculi were removed by RIRS, whereas larger stones required pyelotomy followed by endoscopic removal.12 In our series, preparations were made for pyelotomy and/or laser lithotripsy in three cases. However, we larger calculi were successfully extracted using a semi-rigid URS and stone basket, aided by the ability to manipulate the renal graft during bench surgery.
Metabolic evaluation was negative in all the donors, and all were asymptomatic. In patients with asymptomatic renal calculi of size <5.7 mm, spontaneous expulsion rates may be as high as 20% with the risk of intervention being as low as 7.1%.13 In cases where an asymptomatic calculus is smaller than 4 mm, the risk of intervention is even lower.14 However, the life-threatening complications that may arise from untreated urolithiasis in the solitary kidney of a recipient on immunosuppression necessitate their removal. None of the donors in our series experienced stone-related events within two years of renal donation.
Conclusion
Despite the limitations of our study, such as its retrospective nature and the small number of cases studied, ex vivo URS has been demonstrated to be a viable option in the management of incidentally detected renal calculi in prospective kidney donors. The size of the calculus is the most important factor in determining the success of the procedure and whether adjunctive procedures such as pyelotomy or laser lithotripsy are required. Larger-scale prospective studies are needed to validate this option for the management of urolithiasis in graft kidneys.
Waheedu Zzaman, Ashik Suresh, Abhinav Veerwal. Calculi in Renal Grafts: A Single Centre Experience with
Ex-Vivo Stone Retrieval and Follow-Up. MMJ. 2025, March. Vol 1 (5).
References
- Cosio FG, Falkenhain ME, Pesavento TE, et al. Patient survival after renal transplantation: II. The impact of smoking. Clin Transplant. 1999;13(4):336-41.
- Ashby VB, Leichtman AB, Rees MA, et al. A Kidney Graft Survival Calculator that Accounts for Mismatches in Age, Sex, HLA, and Body Size. Clin J Am Soc Nephrol. 2017;12(7):1148- 1160.
- Scales CD Jr, Smith AC, Hanley JM, et al. Urologic Diseases in America Project. Prevalence of kidney stones in the United States. Eur Urol. 2012;62(1):160-5.
- Stravodimos KG, Adamis S, Tyritzis S, et al. Renal transplant lithiasis: analysis of our series and review of the literature. J Endourol. 2012;26(1):38-44.
- Delmonico F. Council of the Transplantation Society. A Report of the Amsterdam Forum On the Care of the Live Kidney Donor: Data and Medical Guidelines. Transplantation. 2005;79(6 Suppl):S53-66.
- Sorokin I, Mamoulakis C, Miyazawa K, et al. Epidemiology of stone disease across the world. World J Urol. 2017;35(9):1301- 1320.
- Challacombe B, Dasgupta P, Tiptaft R, et al. Multimodal management of urolithiasis in renal transplantation. BJU Int. 2005;96(3):385-9.
- Shim KH, Choi KB, Kim WB, et al. Korean Society of Endourology and Robotics (KSER) Research Committee. Urolithiasis in Kidney Transplant Patients: A Multicenter KSER Research Series. Medicina (Kaunas). 2024;60(1):132.
- Pearle MS, Lingeman JE, Leveillee R, et al. Prospective, randomized trial comparing shock wave lithotripsy and ureteroscopy for lower pole caliceal calculi 1 cm or less. J Urol. 2005;173(6):2005-9.
- Coleman AJ, Saunders JE, Crum LA, et al. Acoustic cavitation generated by an extracorporeal shockwave lithotripter. Ultrasound Med Biol. 1987;13(2):69-76.
- Jan MY, Sharfuddin A, Mujtaba M, et al. Living Donor Gifted Lithiasis: Long-Term Outcomes in Recipients. Transplant Proc. 2021;53(3):1091-1094.
- Pushkar P, Agarwal A, Kumar S, et al. Endourological management of live donors with urolithiasis at the time of donor nephrectomy: a single center experience. Int Urol Nephrol. 2015;47(7):1123-7.
- Koh LT, Ng FC, Ng KK. Outcomes of long-term follow-up of patients with conservative management of asymptomatic renal calculi. BJU Int. 2012;109(4):622-5.
- Burgher A, Beman M, Holtzman JL, et al. Progression of nephrolithiasis: long-term outcomes with observation of asymptomatic calculi. J Endourol. 2004;18(6):534-9.