

Abstract: Contamination of blood cultures can lead to diagnostic confusion and increased healthcare costs due to unnecessary treatments and tests. Various techniques have been explored to reduce contamination rates, addressing the challenge of distinguishing true pathogens from contaminants. This study offers an overview of blood culture contamination, examining different approaches for enhancing both detection and prevention. It emphasizes the need for multidisciplinary collaboration and diverse strategies to enhance the accuracy and quality of blood culture sampling.
Initiatives to improve infection control practices aim to ensure patient safety and achieve better outcomes. An observed increase in blood culture contamination rates in the Emergency department prompted our efforts to scientifically improve sampling methods and decrease colonizer blood culture reports.
Key words: Blood Cultures, Colonisation, Aseptic Techniques
Introduction
Contamination of blood cultures presents challenges for clinicians and microbiologists in diagnosing sepsis. It leads to diagnostic uncertainty and increased healthcare costs, necessitating multidisciplinary efforts and multitargeted strategies to improve blood culture sampling quality and reliability.[1]
Background
Surveillance data, Infection Control Nurse (ICN) audits, and feedback from Intensive Care Unit (ICU) clinicians have highlighted an increasing trend of contaminated blood cultures in the Emergency department.
Aim & objectives
Blood culture contamination poses risks for patients, including unnecessary antimicrobial therapy and additional hazards and costs. One effective method to reduce contamination is initial blood specimen diversion during collection. Our project aimed to:
1. Enhance safe sampling practices in the Emergency department.
2. Identify gaps in techniques and practices.
3. Plan and implement corrective and preventive actions.
4. Strengthen processes.
Definition of contaminated/colonizer blood culture
Contaminated blood culture refers to the presence of commensal and environmental organisms in a single blood culture set, not indicative of true bacteremia.[1]
Colonization: Presence of a microorganism on/in a host, with growth and multiplication of the organism, but without interaction between host and organism (no clinical expression, no immune response).[1]
Impacts of colonizer report:
1. Compromise patient care quality.
2. Unnecessary antibiotic exposure.
3. Prolonged hospitalization.
4. Induce mental stress to the patient and healthcare personnel.
Methods
A retrospective study conducted from January 2023 to June 2023 involving 1306 patients identified 46 cases of coagulase-negative staphylococcus positive blood cultures (Figure 1). The Define, Measure, Analyze, Improve and Control (DMAIC) process was followed to define the process, measure the baseline rate, identify issues by using audit checklist (Figure 2), analyse the data, identify root causes, implement corrective and preventive actions, and ensure sustainability. Root cause analysis was conducted using the 5 Whys and fish bone method (Figure 3).
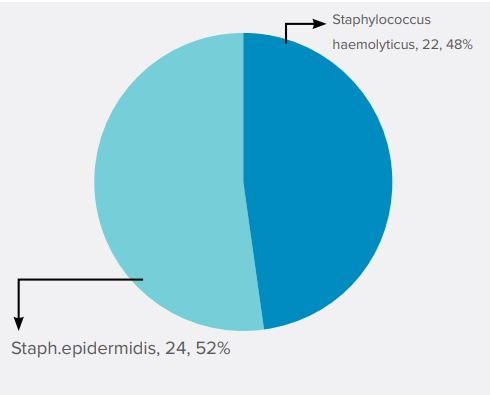
Figure 1: Rate of colonizer report-46 Patients positive with (Jan’23 to Jun’23)
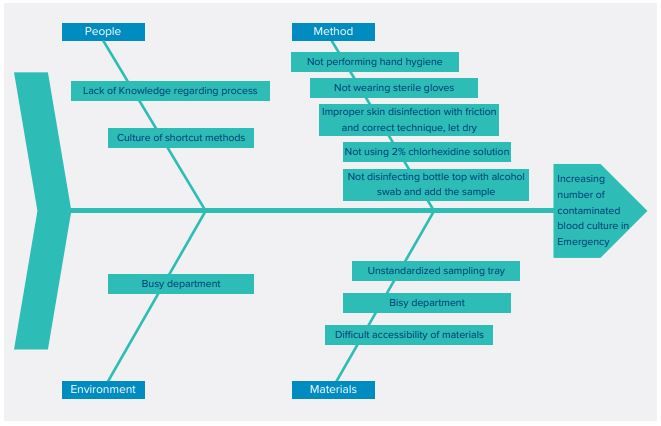
Figure 3: Fish bone analysis
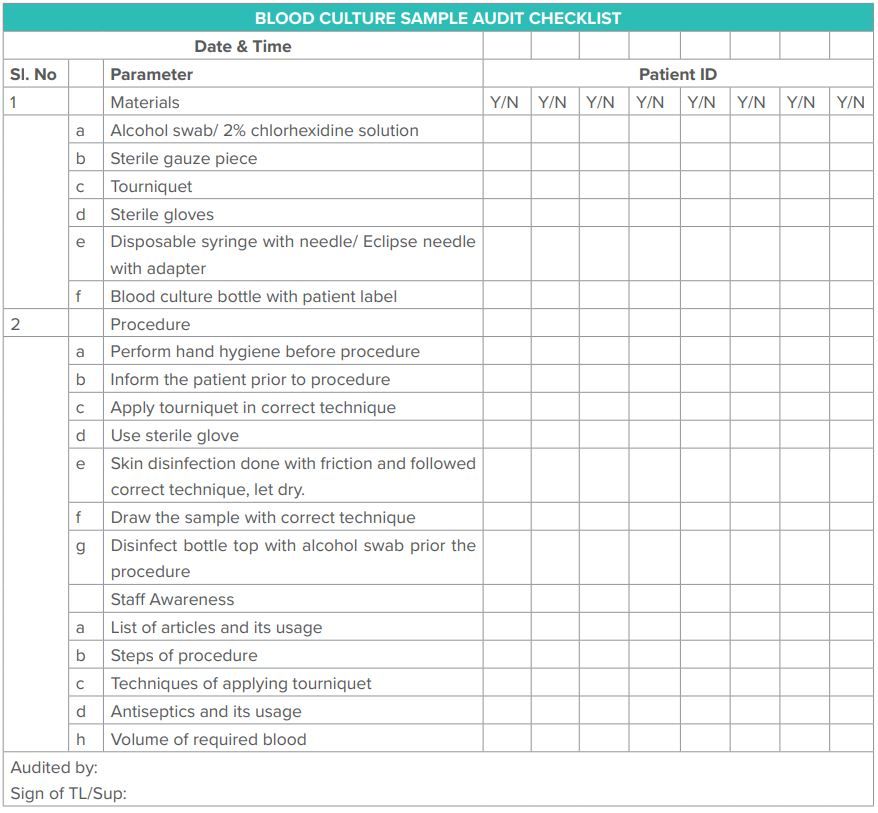
Figure 2: Audit checklist
Critical findings in fish bone analysis
1. Aseptic technique and hand hygiene were not followed before the procedure.
2. Sterile gloves were not used.
3. Proper technique of skin preparation, including drying, was not followed.
4. 2% w/v Chlorhexidine Gluconate (CHG) was not utilized.
5. Tourniquet was not disinfected between patients.
6. Bottle tops were not disinfected.
7. Insufficient articles were present in the tray.
8. There was no standardized blood culture sampling tray.
Corrective action & preventive action[2,3]
1. Implemented standardized blood culture sampling tray.
2. Initiated 2-step skin preparation: first step with alcohol swab and second step with 2% w/v CHG.
3. Standardized the list of articles for blood culture sampling.
4. Prepared a flow chart outlining the steps of blood culture sampling, incorporating correct practices as per CDC guidelines and evidence-based studie.[4]
5. Conducted training for staff on the implemented initiatives.
Result
A comparative study was conducted to evaluate the efficacy of using 70% isopropyl alcohol alone versus a combination of 2% chlorhexidine product with 70% isopropyl alcohol for skin preparation, alongside the DMAIC process. Initially, only 70% isopropyl alcohol was used for skin preparation in 709 patients from July 2023 to September 2023, but the rate of colonizer reports remained unchanged. Consequently, starting from October 2023, a combination of 2% chlorhexidine product and 70% isopropyl alcohol was adopted for skin and blood culture bottle septum disinfection, respectively. This was followed by the collection of two or more blood culture sets from separate peripheral venepuncture sites, newly inserted IV catheters, or line draws when clinically indicated. A standard definition of a contaminant due to skin flora, specifically coagulase-negative staphylococcus, was utilized. A total of 649 patients in this phase experienced a reduction in contaminated blood culture reports. Our project achieved a 57 % reduction in contaminated /colonizer report (Table 1&2).

Table 1: Rate of contaminated/ colonizer blood culture report [Pre, intra and post project]
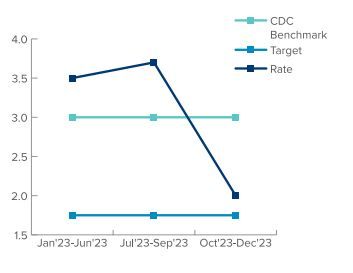
Table 2: Trend of contaminated/ colonizer blood culture report [Pre, intra and post project]
CONCLUSION:
Implementation of standardized blood culture trays with 2%w/v CHG, development of procedural flow charts, and comprehensive staff training, significantly improved practices and staff knowledge. Notably, the project also addressed the requirement of correct blood volume sampling.

References
- Bates DW, Goldman L, Lee TH. Contaminant blood cultures and resource utilization: the true consequences of false-positive results. Jama. 1991 Jan 16;265(3):365-9.
- Patton RG, Schmitt T. Innovation for reducing blood culture contamination: initial specimen diversion technique. Journal of clinical microbiology. 2010 Dec;48(12):4501-3.
- Binkhamis K, Forward K. Effect of the initial specimen diversion technique on blood culture contamination rates. Journal of clinical microbiology. 2014 Mar;52(3):980-1.
- CDC. Blood Culture Contamination: An Overview for Infection Control and Antibiotic Stewardship Programs Working with the Clinical Laboratory [Internet]. Available from: https://www.cdc.gov/antibiotic-use/core-elements/ pdfs/fs-bloodculture-508.
- Salluzzo R, Reilly K. The rational ordering of blood cultures in the emergency department. American Journal of Medical Quality. 1991 Mar 1;6(1):28-31.