

Abstract:
Adrenocortical carcinoma (ACC) is a rare, aggressive malignancy with high recurrence rates even after complete resection. The role of adjuvant therapy remains controversial, owing to the scarcity of prospective data and disease heterogeneity. This article synthesises current evidence regarding the efficacy, indications, and evolving role of adjuvant mitotane and radiotherapy in resected ACC. A comprehensive literature review was conducted encompassing retrospective analyses, multi-institutional studies, meta-analyses, and recent prospective trials evaluating adjuvant mitotane and radiotherapy in ACC. Studies were analysed for recurrence-free survival (RFS), overall survival (OS), and toxicity outcomes. Mitotane, the only approved systemic therapy for ACC, shows benefit primarily in high-risk patients (European Network for the Study of Adrenal Tumours [ENSAT] stage III, R1 resection, Ki-67 > 10%). The ADIUVO trial demonstrated no significant improvement in RFS or OS for low- to intermediate-risk disease, supporting a risk-adapted approach. Ongoing trials (ACACIA, ADIUVO-2) are exploring combination chemotherapy with mitotane in higher-risk cohorts. Increasing evidence supports adjuvant radiotherapy (RT) in improving locoregional control, particularly in margin-positive or locally advanced cases. Meta-analyses confirm significant reductions in locoregional recurrence (Hazard ratio [HR] ≈ 0.34) and improvements in OS (HR ≈ 0.6), with modern conformal RT demonstrating favourable toxicity profiles. Adjuvant therapy remains critical in optimising outcomes for high-risk resected ACC, with current data supporting selective mitotane use and adjuvant RT in appropriately chosen patients. Future prospective, risk-stratified trials integrating systemic and locoregional modalities are essential to refine treatment paradigms and improve survival in this rare malignancy.
Key words: Adrenocortical Carcinoma, Mitotane, Adjuvant Radiotherapy, Recurrence-Free Survival, ENSAT, High-Risk.
Background
Adrenocortical carcinoma (ACC) is a rare and aggressive malignant tumour of the adrenal cortex, with an incidence of approximately 1–2 cases per million population annually.1-3 It is more common in women (55%–65%) than in men (35%–45%) and exhibits a heterogeneous clinical behaviour that can range from indolent growth to rapid progression.4 In contrast to benign adrenal tumours — which are among the most common human neoplasms with a prevalence exceeding 3% in adults over 50 years — ACC carries a markedly poor prognosis.5 Reported 5-year survival rates vary significantly with disease stage: 65%–82% for European Network for the Study of Adrenal Tumours (ENSAT) stage I, 58%–68% for stage II, 41%–55% for stage III, and only 10%–20% for stage IV disease.3,6
Complete surgical excision remains the primary curative approach for localised and selected locally advanced disease. Despite complete macroscopic resection, recurrence in ACC remains alarmingly common. Reported rates after adrenalectomy range from 60% to 80%, underscoring the aggressive biology of the disease. Even when negative surgical margins are achieved, up to one-third of patients will develop local recurrence. The risk is substantially higher in cases with positive margins, where local failure rates can reach approximately 60%.7-9
This has fuelled interest in adjuvant therapies aimed at reducing relapse risk and improving survival outcomes. Mitotane, an adrenolytic agent, has long been used in the adjuvant setting, supported by retrospective analyses and some prospective data, though its optimal use, duration, and patient selection remain subjects of debate. Additionally, radiotherapy — once considered of limited value in ACC — has gained attention in select high-risk postoperative patients, particularly those with margin positivity or adverse pathological features, with emerging evidence suggesting improved local control.
In this review, we summarise current evidence and expert perspectives on adjuvant therapy in ACC, discuss key prognostic factors influencing treatment decisions, and outline evolving strategies that aim to improve patient outcomes in this challenging malignancy.
Risk Stratification3
Low risk: ENSAT stage I or II and Ki-67≤ 10%
Standard risk: ENSAT stage I or II and Ki-67 between 11% and 30%, or ENSAT stage III and Ki-67 < 30%.
Very high risk: Any of the following:
- Ki-67 ≥ 30%
- Large tumour thrombus in the vena cava
- Stage IV
- R1 resection
Prognostication3
The Grade, Resection Status, Age, and Symptoms (GRAS) score is used. A modified version of this score also includes stage (S-GRAS).
Stage:
- The risk of relapse at 5 years is estimated at 18%–47%, 36%–62%, 50%–81%, respectively, for stages 1, 2, or 3.
- The 5-year survival varies according to the stages, from 63%–88% for stages 1 to 38%–73% for stage 2, 19%–54% for stage 3, and 0%–21% for stage 4.
- Recent data show that nodal involvement has an unfavourable prognosis identical to stage 4.
Grade (Weiss score/Ki-67):
- Higher Ki-67 levels are consistently associated with poor prognosis.
- Threshold levels of 10% and 20% have been considered for discriminating low from high Ki-67 labelling indices.
- Weiss score > 6 is considered high (The Weissscore is a histopathological scoring system used to assess the malignant potential of adrenocortical tumours).
Resection: Positive surgical margins (R1 resection) are a risk factor for worse outcomes in ACC and are associated with shorter overall survival (OS) and recurrence-free survival (RFS) compared to patients with negative margins (R0 resection).
Age: Age is an independent prognostic factor; older adults (more than 50 years of age) usually have a poorer prognosis.
Symptoms:
- Hormonally functional status is a predictor of poor prognosis.
- Of all the types of hormonally active tumours, glucocorticoid tumours have the poorest prognosis.
Current Evidence
Role of mitotane:
Mitotane is an adrenolytic drug with selective toxicity toward adrenal cortical cells. To date, the only drug specifically approved for the treatment of ACC is mitotane. It acts by inhibiting adrenal cortical function, both through direct suppression and, in some cases, by causing cellular destruction. It is a derivative of the insecticide dichlorodiphenyltrichloroethane (DDT), is currently the only drug specifically approved for the treatment of ACC. Its pharmacologic effects include suppression of corticosteroid synthesis and alteration of peripheral steroid metabolism, resulting in increased urinary excretion of 17-hydroxycorticosteroids and 17-ketosteroids.10
The role of mitotane following curative-intent surgery for ACC continues to generate debate, largely due to the scarcity of high-quality prospective data. Interpretation of available studies is often complicated by methodological limitations and patient selection biases.11
A retrospective analysis was conducted involving 207 patients who underwent resection of ACC at 13 institutions across the United States, of whom 88 received adjuvant mitotane. In this cohort, adjuvant mitotane was associated with shorter RFS and OS. However, causality could not be established, as the mitotane group appeared to have a higher baseline risk of recurrence, reflecting treatment selection bias, which could not be completely accounted for despite statistical adjustment.12
A multicentre, case–control study was conducted in Italy and Germany, which compared outcomes of 47 patients treated at four Italian centres where adjuvant mitotane was routinely administered with two control groups: 55 patients from other Italian centres and 75 from German centres where adjuvant therapy was not standard practice. A key methodological strength was that treatment allocation was based on institutional policy rather than individual patient characteristics, minimising selection bias. Baseline characteristics were well matched between the mitotane group and the first control group, although the second control group included older patients and a greater proportion with early-stage disease. With a median follow-up exceeding 10 years, median RFS was significantly longer in the mitotane group (42 months) compared with control group 1 (17 months) and control group 2 (26 months). Median OS was also significantly prolonged compared with control group 1 (161 vs 65 months), although the difference versus control group 2 (92 months) did not achieve statistical significance.13,14
The most definitive prospective evidence comes from the ADIUVO trial (NCT00777244) , the first and only randomised controlled study on adjuvant mitotane in ACC. This multicentre, open-label, Phase III trial enrolled patients with completely resected, low- to intermediaterisk ACC (ENSAT stage I–III, R0 resection, Ki-67 ≤ 10%) and randomised them to adjuvant mitotane for two years or active surveillance. Due to slow accrual, only 91 patients were randomised (45 mitotane, 46 surveillance) over a decade, leaving the trial underpowered. At a median follow-up of 48 months, 5-year RFS was 79% with mitotane and 75% with surveillance (hazard ratio [HR] 0.74, 95% confidence interval [CI] 0.30–1.85), while 5-year OS was 95% versus 86% (HR 0.46, 95% CI 0.08–1.92) — differences that were not statistically significant. Recurrence occurred in 16% of mitotane-treated patients versus 24% under surveillance. No subgroups showed a clear differential benefit. A parallel prospective observational cohort of 95 patients managed according to patient preference confirmed these findings. The ADIUVO trial demonstrated that in patients with low-grade, localised ACC at low to intermediate recurrence risk, prognosis with surveillance alone is favourable, with 5-year RFS approaching 75%. In this group, the modest and non-significant differences in outcomes, combined with mitotane’s toxicity, suggest that routine use is unwarranted. These findings, however, should not be extrapolated to higher-risk ACC, where adjuvant mitotane remains supported by retrospective evidence and expert consensus guidelines.15
While retrospective analyses and the ADIUVO trial have shaped current practice, ongoing trials aim to address key gaps in evidence and refine adjuvant treatment strategies for ACC.
The ACACIA trial (NCT03723941) is a Phase II randomised controlled study involving patients with localised, resected ACC (ENSAT stages I–III), stratified by recurrence risk. It compares the standard of care — which may be observation or mitotane — with combination therapy using etoposide, cisplatin, and mitotane (EP-M). The primary endpoint is disease-free survival (DFS). ACACIA seeks to determine whether early systemic therapy can confer benefit even in localised disease, potentially expanding the role of combination chemotherapy beyond high-risk groups.16
The ADIUVO-2 trial (NCT03583710) is a Phase III, randomised, international registry study enrolling high-risk patients after complete resection — such as those with R0/R1 resection, Ki-67 > 10%, or ENSAT stage III disease. Participants are randomised to receive either adjuvant mitotane alone or mitotane combined with platinum-based chemotherapy (cisplatin and etoposide). The primary endpoint is RFS. By focusing on a population at the highest risk of relapse, ADIUVO-2 is expected to provide the first prospective evidence on whether adding systemic chemotherapy to mitotane improves outcomes compared with mitotane monotherapy.17
Together, these studies are expected to clarify the optimal role of mitotane monotherapy versus combination regimens, help define risk-adapted strategies, and guide future guideline recommendations.
Considerations in the use of adjuvant mitotane:
Mitotane therapy in ACC is associated with several practical challenges that influence its use in the adjuvant setting. Access can be limited due to its manufacture by only a few companies and restricted distribution pathways, which may delay treatment initiation. The drug has a narrow therapeutic window, necessitating regular plasma level monitoring to ensure efficacy while avoiding toxicity. Adverse effects are frequent and often significant, including gastrointestinal intolerance, neurotoxicity, hepatotoxicity, dyslipidaemia, skin changes, and endocrine disturbances that may require long-term hormone replacement. Its long halflife results in a delayed onset of action, with therapeutic levels sometimes taking weeks to months to achieve, which can be problematic in patients with rapidly progressive disease. Furthermore, the need for frequent laboratory monitoring, careful dose adjustments, and multidisciplinary follow-up, coupled with its impact on quality of life — such as fatigue and cognitive changes — makes patient selection and counselling essential before initiating mitotane.11
Role of radiation therapy:
While ACC has long been considered relatively resistant to radiation, emerging data challenge this perception.
At MD Anderson Cancer Center, Habra et al. retrospectively analysed 58 patients with ACC treated between 1983 and 2011, of whom 20 received adjuvant radiotherapy (RT) after surgical resection. The primary aim was to evaluate the impact of postoperative RT on local recurrence-free survival (LRFS). Patients in the RT group had more adverse features, including higher stage and positive or close margins, compared with those managed with surgery alone. Despite these imbalances, adjuvant RT was associated with a significantly reduced risk of local recurrence (3-year LRFS 79% vs 45%, p = 0.03) and a non-significant trend toward improved OS. Toxicity was generally mild to moderate, with no unexpected late effects. The authors concluded that postoperative RT should be considered in patients at elevated risk of locoregional relapse, particularly those with margin-positive resections.18
Sabolch et al. conducted a multi-institutional retrospective analysis encompassing 360 patients from 13 United States (U.S.) centres, of whom 58 received adjuvant RT after complete macroscopic resection. The study sought to determine whether RT conferred a local control or survival advantage. Using propensity score matching to balance high-risk factors between groups, adjuvant RT significantly improved locoregional control (LC) (5-year LC 76% vs 44%, p < 0.001) and demonstrated a trend toward improved disease-specific survival. The benefit was most notable in patients with ENSAT stage III disease or R1 margins. Acute toxicity was primarily grade 1–2 gastrointestinal or constitutional symptoms, and severe late toxicity was rare, reflecting the adoption of modern conformal techniques.19
Nelson et al. analysed the National Cancer Data Base (NCDB) data from 2004–2013 to assess the impact of adjuvant RT in non-metastatic ACC following surgery. Among 1,184 patients identified, 171 (14.4%) received adjuvant RT. While demographic characteristics were similar between groups, those receiving RT were significantly more likely to have positive margins (37.4% vs 14.6%; p < 0.001), vascular invasion (14.0% vs 5.1%; p = 0.05), and concurrent chemotherapy (57.3% vs 28.8%; p < 0.001). On multivariable analysis, positive margin status was the only independent predictor of RT use (odds ratio [OR] 3.84, 95% CI 1.95–7.56). In the overall cohort, RT was not associated with improved median OS; however, in the subset with positive margins, adjuvant RT reduced the yearly risk of death by 40% after adjustment for chemotherapy use (HR 0.60, 95% CI 0.40–0.92; p = 0.02). No survival benefit was observed for other traditional high-risk features. The authors concluded that adjuvant RT should be considered in multidisciplinary planning for patients with margin-positive ACC, although its utilisation in the U.S. remains limited.20
At the University of Michigan Endocrine Oncology Program, Gharzai et al. performed a retrospective, propensity-matched cohort study to evaluate the impact of adjuvant RT following adrenalectomy for ACC. Of 424 patients screened, 78 were included — 39 who received RT and 39 matched controls — matched by age, tumour stage, grade, surgical margin status, and adjuvant mitotane use. RT targeted the tumour bed with or without regional lymph nodes, with a median dose of 55 Gy (range 45–60 Gy). Adjuvant RT was associated with significantly improved LRFS (p = 0.002), DFS (p = 0.0035), and OS (p = 0.0024) compared with matched controls. The authors emphasised that RT should be considered within a multidisciplinary framework, particularly for patients with high-risk pathological features, incomplete resection margins, or large primary tumours.21
Wu and colleagues performed a retrospective singlecentre study of 105 patients with localised ACC treated from 2015 to 2021; 46 patients (43.8%) received adjuvant RT within three months of surgery, and 59 underwent surgery alone. Median follow-up was 36.5 months (interquartile range [IQR] 19.7–51.8). RT was delivered with intensity-modulated techniques to the tumour bed (median dose 45.0 Gy, range 30.0–50.4 Gy), and patients were matched on margin status and stage for comparisons. At 3 years, OS was higher in the RT group (87.9% vs 79.5%; log-rank p = 0.039), and median DFS increased from 16.5 months (no RT) to 34.6 months (RT) (log-rank p = 0.033). Recurrence rates were lower with RT (50.0% vs 78.0%; p = 0.003), and fewer deaths occurred in the RT arm (5 vs 20; p = 0.006). On multivariable Cox modelling (adjusting for ENSAT stage and Ki-67), adjuvant RT remained independently associated with improved OS (adjusted HR 0.293, 95% CI 0.107–0.798; p = 0.016) but did not show an independent benefit for DFS after adjustment (p = 0.164). Toxicities were mostly mild–moderate (Radiation Therapy Oncology Group [RTOG]/ Common Terminology Criteria for Adverse Events [CTCAE]), with six grade-3 events documented (one grade-3 intestinal event and five grade-3 leucopenias). Subgroup analyses suggested the survival and DFS benefit was particularly evident in patients with ENSAT I–II disease. The authors concluded that adjuvant RT was associated with better survival and longer DFS in their cohort and was generally well tolerated.22
Tsuboi and colleagues conducted a systematic review and meta-analysis to clarify the role of RT in patients with ACC following surgery. A total of seven retrospective studies were included, encompassing 1,249 patients, of whom 277 received adjuvant RT. Across the pooled data, adjuvant RT was associated with a significant improvement in locoregional RFS (HR 0.34, 95% CI 0.23–0.51, p < 0.001) and OS (HR 0.60, 95% CI 0.45–0.81, p = 0.001) compared to surgery alone. The benefit in DFS did not reach statistical significance in the overall cohort (HR 0.78, 95% CI 0.57–1.06, p = 0.11). Subgroup analyses indicated the greatest OS benefit in patients with positive margins or advanced-stage disease. The authors acknowledged the limitations of relying solely on retrospective data, including potential selection bias, heterogeneity in RT doses and techniques, and variable use of concurrent/adjuvant mitotane. Nonetheless, they concluded that adjuvant RT appears to offer meaningful LC and survival advantages in selected high-risk ACC patients.23
A summary of key studies evaluating the impact of adjuvant radiotherapy in ACC is presented in Table 1.
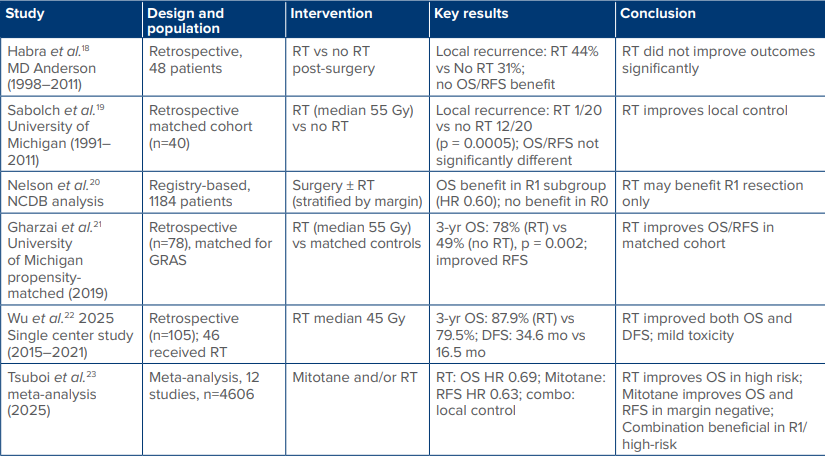
Table 1: Evidence base for the role of adjuvant radiotherapy in adrenocortical carcinoma
Abbreviations: DFS: Disease-Free Survival; GRAS: Grade, Resection Status, Age, and Symptoms; HR: Hazard Ratio; mo: Months; NCDB: National Cancer Data Base; OS: Overall Survival; RFS: Recurrence-Free Survival; RT: Radiotherapy; yr: Year.
Evolving Perspectives
The management of ACC has witnessed a gradual but meaningful shift over the past two decades. While surgical resection remains the cornerstone of treatment for localised disease, the high recurrence rates — especially in patients with adverse prognostic features — have prompted increasing interest in multimodality strategies. Historically, adjuvant mitotane was the main systemic option, despite limited prospective data and challenges related to its narrow therapeutic window, toxicity profile, and prolonged time to achieve effective plasma concentrations. The recent ADIUVO trial refined its role by showing no survival advantage in low- to intermediate-risk patients, thereby underscoring the need for patient selection and reserving mitotane monotherapy for higher-risk cohorts as per ENSAT and National Comprehensive Cancer Network (NCCN) recommendations.
Parallel to systemic therapy, adjuvant RT has emerged from a controversial adjunct to a more widely discussed component of multidisciplinary care. Early singleinstitution series suggested improved LC in high-risk patients, but concerns about retrospective bias and heterogeneity in technique limited broader adoption. In recent years, multi-institutional studies, propensitymatched analyses, and pooled meta-analyses have provided stronger evidence supporting RT’s role, particularly in patients with positive surgical margins, large tumours, or high-grade histology. Improved RT technology, including conformal planning and image-guided delivery, has mitigated some of the toxicity concerns historically associated with adrenal bed irradiation. Consequently, contemporary perspectives increasingly view RT as a tailored option for selected high-risk patients rather than as a blanket recommendation.
Another evolving area is the integration of combined adjuvant modalities. Data remain sparse on the synergistic or additive effects of mitotane and RT, but ongoing studies — such as ADIUVO-2 — are expected to clarify whether concurrent or sequential use can improve outcomes in patients at higher risk of recurrence. Molecular profiling and biomarkers may further refine adjuvant treatment strategies in the future, enabling risk-adapted therapy that balances efficacy with quality of life.
Recommendations as per Guidelines
Adjuvant RT plays a selective but important role in the management of ACC. According to expert consensus and institutional practice, RT is considered in cases where surgical resection is incomplete — either microscopically (R1) or macroscopically (R2) — as well as in the postoperative setting after local recurrence has been re-resected. RT is also preferred in patients with localised disease, restricted spread, or tumour capsule rupture, particularly when re-operation would be technically challenging or not feasible. However, RT is typically avoided in the presence of widespread metastatic disease due to limited therapeutic benefit in that context.
The NCCN Guidelines (Version 2.2025) recommend considering external beam radiation therapy (EBRT) to the tumour bed in patients at high risk for local recurrence. High-risk features include positive surgical margins, Ki-67 proliferation index greater than 10%, tumour rupture, large tumour size, and high-grade histology. In such patients, RT may serve as an important adjuvant modality to reduce the likelihood of local recurrence, although its use should be individualised based on patient factors and institutional expertise.
Mitotane is another adjuvant therapy option in ACC, especially for patients at high risk of recurrence. The NCCN guidelines recommend considering adjuvant mitotane therapy as a Category 3 recommendation in these settings. Mitotane therapy requires close monitoring, as therapeutic levels (typically 14–20 mcg/mL) may take several months to achieve, and its use is associated with significant adrenal suppression. Therefore, patients on mitotane usually require lifelong hormone replacement with hydrocortisone and/or fludrocortisone. While mitotane may offer greater benefit in controlling hormonerelated symptoms, its role in directly controlling tumour progression remains uncertain, and its use is often guided by institutional experience and patient tolerance.
Conclusion
ACC remains a rare but aggressive malignancy with a persistently high risk of recurrence despite optimal surgery. Adjuvant therapy plays a pivotal role in improving outcomes for patients with high-risk features. Current evidence supports the selective use of mitotane in patients with adverse prognostic indicators, guided by ENSAT and NCCN recommendations, while the role of adjuvant RT is increasingly supported by retrospective and pooled analyses, particularly in margin-positive or locally advanced cases. The heterogeneity of available data, coupled with the rarity of the disease, highlights the ongoing need for collaborative multicentre efforts, prospective trials, and standardised treatment protocols.
As the therapeutic landscape evolves, the emphasis is shifting toward personalised adjuvant strategies — matching treatment intensity to recurrence risk, optimising tolerability, and integrating advances in systemic therapy, radiotherapy, and molecular oncology. Until robust prospective evidence becomes available, clinical decision-making should remain multidisciplinary, incorporating surgical, medical oncology, and radiation oncology expertise to individualise adjuvant treatment for each patient with ACC.
Declaration of the use of artificial intelligence (AI) in the writing process
During the preparation of this work, the authors used AI tools only for language editing and grammar refinement. No generative AI was employed to create, analyse, or interpret the scientific content. The authors reviewed and verified all text to ensure accuracy and integrity, and take full responsibility for the final content of the manuscript.
Ajinkya Gupte, Kaustav Talapatra, Hemant Tongaonkar. Adjuvant Therapy in Adrenocortical Carcinoma: Review of Evidence and Evolving Perspectives. MMJ. 2025, December. Vol 2 (4).
References
- Kerkhofs TM, Verhoeven RH, Van der Zwan JM, et al. Adrenocortical carcinoma: a population-based study on incidence and survival in the Netherlands since 1993. Eur J Cancer. 2013;49(11):2579–86.
- Pedersen J, Jarløv AE, Rasmussen ÅK, et al. Incidence, Treatment, and Survival of Adrenocortical Carcinoma in Denmark 2003-2019. J Endocr Soc. 2024;8(3):bvae012.
- Fassnacht M, Puglisi S, Kimpel O, et al. Adrenocortical carcinoma: a practical guide for clinicians. Lancet Diabetes Endocrinol. 2025;13(5):438–52.
- Jasim S, Habra MA. Management of Adrenocortical Carcinoma. Curr Oncol Rep. 2019;21(3):20.
- Fassnacht M, Arlt W, Bancos I, et al. Management of adrenal incidentalomas: European Society of Endocrinology Clinical Practice Guideline in collaboration with the European Network for the Study of Adrenal Tumors. Eur J Endocrinol. 2016;175(2):G1–34.
- Puglisi S, Calabrese A, Ferraù F, et al. New Findings on Presentation and Outcome of Patients With Adrenocortical Cancer: Results From a National Cohort Study. J Clin Endocrinol Metab. 2023;108(10):2517–25.
- Meyer A, Behrend M. Long-term survival over 28 years of a patient with metastatic adrenal cortical carcinoma--case report. Anticancer Res. 2004;24(3b):1901–4.
- Else T, Kim AC, Sabolch A, et al. Adrenocortical Carcinoma. Endocr Rev. 2014;35(2):282–326.
- Tsuboi I, Kardoust Parizi M, Matsukawa A, et al. The efficacy of adjuvant mitotane therapy and radiotherapy following adrenalectomy in patients with adrenocortical carcinoma: A systematic review and meta-analysis. Urol Oncol. 2025;43(5):297–306
- Hogan TF, Citrin DL, Johnson BM, et al. o,p’-DDD (mitotane) therapy of adrenal cortical carcinoma: observations on drug dosage, toxicity, and steroid replacement. Cancer. 1978;42(5):2177–81
- Shirley M. Mitotane in adrenocortical carcinoma: a profile of its use. Drugs & Therapy Perspectives. 2022;38(12):508–19.
- Postlewait LM, Ethun CG, Tran TB, et al. Outcomes of adjuvant mitotane after resection of adrenocortical carcinoma: a 13-institution study by the US Adrenocortical Carcinoma Group. J Am Coll Surg. 2016;222(4):480–90.
- Berruti A, Grisanti S, Pulzer A, et al. Long-term outcomes of adjuvant mitotane therapy in patients with radically resected adrenocortical carcinoma. J Clin Endocrinol Metab. 2017;102(4):1358–65.
- Terzolo M, Angeli A, Fassnacht M, et al. Adjuvant mitotane treatment for adrenocortical carcinoma. N Engl J Med. 2007;356(23):2372–80.
- Terzolo M, Fassnacht M, Perotti P, et al. Adjuvant mitotane versus surveillance in low-grade, localised adrenocortical carcinoma (ADIUVO): an international, multicentre, open-label, randomised, phase 3 trial and observational study. Lancet Diabetes Endocrinol. 2023;11(10):720–30.
- Study Details. Adjuvant Chemotherapy vs. Observation/Mitotane After Primary Surgical Resection of Localized Adrenocortical Carcinoma. ClinicalTrials.gov [Internet]. [cited 2025 Aug 11]. Available at: https://clinicaltrials.gov/study/NCT03723941. Accessed on: 11th August 2025.
- Mitotane With or Without Cisplatin and Etoposide After Surgery in Treating Patients With Stage I-III Adrenocortical Cancer With High Risk of Recurrence. ClinicalTrials.gov [Internet]. Available at: https://clinicaltrials.gov/study/NCT03583710. Accessed on: 11th August 2025.
- Habra MA, Ejaz S, Feng L, et al. A retrospective cohort analysis of the efficacy of adjuvant radiotherapy after primary surgical resection in patients with adrenocortical carcinoma. J Clin Endocrinol Metab. 2013;98(1):192–7.
- Sabolch A, Else T, Griffith KA, et al. Adjuvant radiation therapy improves local control after surgical resection in patients with localized adrenocortical carcinoma. Int J Radiat Oncol Biol Phys. 2015;92(2):252–9.
- Nelson DW, Chang SC, Bandera BC, et al. Adjuvant Radiation is Associated with Improved Survival for Select Patients with Non-metastatic Adrenocortical Carcinoma. Ann Surg Oncol. 2018;25(7):2060–6.
- Gharzai LA, Green MD, Griffith KA, et al. Adjuvant Radiation Improves Recurrence-Free Survival and Overall Survival in Adrenocortical Carcinoma. J Clin Endocrinol Metab. 2019;104(9):3743–50.
- Wu L, Chen J, Su T, et al. Efficacy and safety of adjuvant radiation therapy in localized adrenocortical carcinoma. Front Endocrinol (Lausanne). 2023;14:1308231.
- Tsuboi I, Kardoust Parizi M, Matsukawa A, et al. The efficacy of adjuvant mitotane therapy and radiotherapy following adrenalectomy in patients with adrenocortical carcinoma: A systematic review and meta-analysis. Urol Oncol. 2025;43(5):297–306.