

Abstract: Extrahepatic portal vein obstruction (EHPVO) is a rare condition that usually affects young adults and is associated with risk of developing non-cirrhotic portal hypertension and portal cholangiopathy. PV recanalisation may be a suitable option in such patients to decompress the portal venous system and help treat portal hypertension and its complications.
Introduction
Extrahepatic portal vein obstruction (EHPVO) is a rare condition that usually affects young adults and often progresses to cavernomatous transformation of the portal vein called portal cavernoma. Non-cirrhotic patients with EHPVO (NC-EHPVO) are at risk of developing pre-hepatic portal hypertension and its associated complications, including gastrointestinal (GI) bleeding, ascites and hypersplenism. In addition, up to 20% of patients with NC-EHPVO develop symptomatic portal cholangiopathy.[1]
Conventionally, these patients are treated by managing the complications of portal hypertension and portal biliopathy (endoscopic variceal management, biliary stenting or surgical shunt creation). Recently, some authors have reported favourable outcomes of transjugular intrahepatic portosystemic shunt (TIPS) placement for treatment of NC-EHPVO.[2] However, in patients without cirrhosis, TIPS may not be necessary, and could potentially contribute to hepatic encephalopathy. Portal vein recanalisation (PVR) without TIPS placement may be a suitable option in such patients which can help reduce portal hypertension. PVR can also improve physiological portal blood perfusion to hepatic parenchyma, unlike TIPS which shunts portal blood away from the liver.
Case: A 9-year-old girl child, known case of EHPVO on regular follow up came to us for upper gastrointestinal endoscopy (UGIE), which revealed high risk varices (GOV1). At the age of 2 years, she has an episode of hematemesis after a brief episode of upper respiratory infection. On evaluation at that time, she was found to have EHPVO, gastroesophageal varices and splenomegaly. She was managed by blood transfusion and endoscopic variceal ligation. There was no history of umbilical vein catheterisation and no obvious developmental delay. Her immunisation is complete till date. Lab values at presentation and one month after PVR are presented in (Table 1).
Review of the contrast CT and doppler ultrasound showed chronically occluded MPV and multiple periportal collateral vessels (Fig 1 a, b). A decision was taken to attempt to recanalise portal vein by interventional radiological techniques. Written consent was obtained after detailed discussions and counselling on the risk and benefits of the procedure.
| Initial values | 1 month after PV recanalisation | |
|---|---|---|
| Haemoglobin | 11.1 | 13.1 |
| Platelets | 105 | 170 |
| TLC | 1.5 | 4.7 |
| Bilirubin (Direct/Indirect) | 0.6 (0.12/0.48) | 0.4 (0.1/0.3) |
| SGOT | 39 | 32 |
| SGPT | 27 | 27 |
| ALP | 126 | 152 |
| PT | 14.6 | 23.4 |
| INR | 1.25 | 2 |
Table 1. Lab values at initial presentation and 1 month after PVR

Figure 1(a): Coronal CT image showing chronically occluded PV with multiple periportal collaterals (arrow). Also note the massive splenomegaly
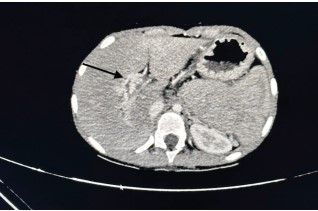
Figure 1(b): Axial CT image shows portal cavernoma in the porta hepatis
Percutaneous transhepatic access of a right portal vein branch was taken under ultrasound guidance. A 6F sheath was placed and a wire/catheter combination (5F KMP catheter, Cookmedical, Bloomington, USA) were used to cross the occluded main portal vein (MPV). A venogram was obtained, which confirmed the occlusion of MPV, presence of multiple periportal collaterals, dilated short gastric veins and varices. MPV was dilated (Fig. 2 a, b, c) with a 7mm diameter balloon (Mustang, Boston Sci, Marlborough, USA). The varices were selectively cannulated and embolised with a thick slurry of mixture of gel foam, sodium tetradecyl sulphate (5%) and lipiodol. Repeat venograms showed satisfactory flow in the main portal vein and disappearance of the periportal collaterals and varices.
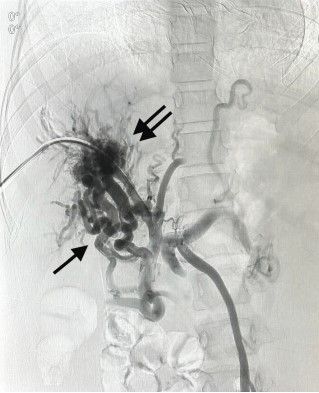
Figure 2(a): DSA of the Porto mesenteric veins shows portal cavernoma (double arrows) and contrast flow in the multiple periportal collateral veins (single arrow)
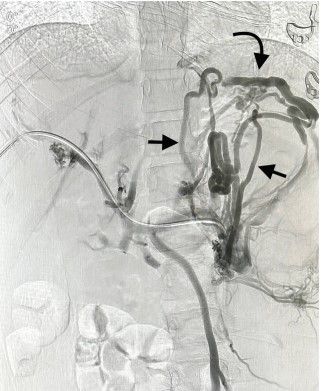
Figure 2(b): Venogram of splenic vein shows multiple dilated short gastric veins (arrows) leading to gastric varices (curved arrow)
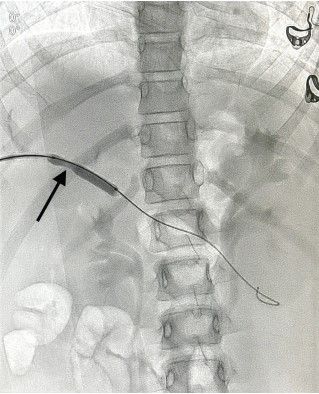
Figure 2(c): Balloon dilation of the MPV shows waist in the balloon
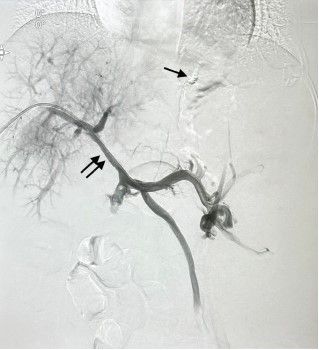
Figure 2(d): DSA after portal vein recanalisation shows flow in MPV (double arrows) and disappearance of the collateral veins (single arrow)
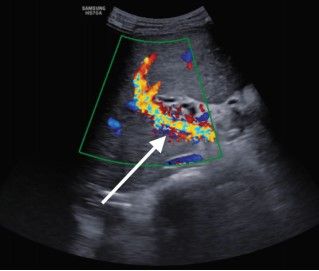
Figure 3: USG doppler after PV recanalisation shows satisfactory flow in the MPV
She was started on oral warfarin. One month later, The ultrasound doppler showed satisfactory portal blood flow (Fig 3). Patient is on regular follow up and there is no repeat episode of GI bleeding or any other complication.
Discussion
EHPVO is predominantly a disease of young age. Patients often present with portal hypertension complications like variceal bleeding. Acute management involves endoscopic variceal ligation. Portal vein recanalisation can reduce portal hypertension, decompress the varices and improve the blood flow to liver. It also provides a chance to antegrade embolise the gastroesophageal varices and thus further reducing the bleeding risk.
Most of the data available on the endovascular approach to portal vein occlusion are derived from studies of patients undergoing liver transplantation or other abdominal surgeries.[3] [4] There is scant literature regarding PV recanalisation in patients with NC-EHPVO.[1][5][6] Additionally, most of the authors have used TIPS insertion[2] in NC-EHPVO and not PV recanalisation alone. Artru et. al, published a study of 31 patients of NC-EHPVO who underwent PV recanalisation without TIPS insertion. They reported a 5-year primary patency of 63% and 73%, for intentionto-treat and per-protocol analysis respectively. Besides, 68% of patients with intention-to-treat analysis and 78% of patients with per-protocol analysis had complete resolution of portal hypertension-related symptoms at 5 years.[1] An earlier study by the same group also reported similar results.[5]
Our case emphasises the feasibility and safety of PVR for the treatment of NC-EHPVO. To the best of our knowledge, this is the first reported case of PVR in paediatric patient with NCEHPVO. The procedure not only helped to reduce the risk of variceal bleeding but also improved the physiological portal flow to liver. In our opinion, PV recanalisation can be an optimal treatment option in carefully selected NC-EHPVO patients.
References
- Artru F, Vietti-Violi N, Sempoux C, Vieira Barbosa J, Becce F, Sah N, Marot A, Deltenre P, Moschouri E, Fraga M, Hocquelet A, Duran R, Moradpour D, Rautou PE, Denys A. Portal vein recanalisation alone to treat severe portal hypertension in non-cirrhotic patients with chronic extrahepatic portal vein obstruction. JHEP Rep. 2022 May 25;4(8):100511. doi: 10.1016/j.jhepr.2022.100511. PMID: 35801087; PMCID: PMC9253474
- Knight GM, Clark J, Boike JR, Maddur H, Ganger DR, Talwar A, Riaz A, Desai K, Mouli S, Hohlastos E, Garcia Pagan JC, Gabr A, Stein B, Lewandowski R, Thornburg B, Salem R. TIPS for Adults Without Cirrhosis With Chronic Mesenteric Venous Thrombosis and EHPVO Refractory to Standardof-Care Therapy. Hepatology. 2021 Nov;74(5):2735-2744. doi: 10.1002/hep.31915. Epub 2021 Jul 8. PMID: 34021505
- Saad WE. Portal interventions in liver transplant recipients. Semin Intervent Radiol. 2012 Jun;29(2):99-104. doi: 10.1055/ s-0032-1312570. PMID: 23729979; PMCID: PMC3444876
- Woodrum D.A., Bjarnason H., Andrews J.C. Portal vein venoplasty and stent placement in the nontransplant population. J. Vasc. Intervent. Radiol. 2009;20:593–599. doi: 10.1016/j.jvir.2009.02.010
- Marot A, Barbosa JV, Duran R, Deltenre P, Denys A. Percutaneous portal vein recanalization using selfexpandable nitinol stents in patients with non-cirrhotic non-tumoral portal vein occlusion. Diagn Interv Imaging. 2019 Mar;100(3):147-156. doi: 10.1016/j.diii.2018.07.009. Epub 2018 Nov 28. Erratum in: Diagn Interv Imaging. 2019 Jun;100(6):389. PMID: 30503174
- Lima da Rocha RD, Diniz PIAR, Leão AG, Rodriguez JER, Campelo PRDS, Souza JEDS, Bernardes MV, Cavalcante LP. Direct portal vein recanalization with stenting associated with embolization of esophagogastric varices in a patient with portal vein thrombosis. Ann Med Surg (Lond). 2022 Sep 2;81:104527. doi: 10.1016/j.amsu.2022.104527. PMID: 36147127; PMCID: PMC9486751