

Abstract: In this case, a 56 years dialysis dependent patient presented with complaints of angina at rest for 2 weeks after which she was thoroughly evaluated and was diagnosed with coronary artery disease with calcified aorta along with calcification of other vessels also, following which she was planned for CABG surgery. The unclampable ascending aorta (UAA) is a condition increasingly encountered during CABG procedures[1]. Aging of the population and the increase in patients on dialysis have led to an increasing frequency of “porcelain aorta”[2]. The use of the no-touch technique is associated with a high perioperative risk but a superior possibility of complete revascularisation, whereas the adoption of the no-pump strategy ensures a smoother postoperative course at the expense of a higher incidence of ischemia recurrence[3]. Enclose-II anastomosis assist device was originally developed as an ancillary device for proximal anastomosis in off-pump coronary artery bypass grafting (OPCABG), to assist anastomosis for the vascular grafts without clamping the ascending aorta[3]
UAA-Unclampable ascending aorta, ENCLOSE II, CKD- Chronic kidney disease, Anastomosis in OPCABG
Introduction
Chronic kidney disease patients have an increased rate and extent of calcification of the intima, media of vessels, heart valves and even of myocardium. In dialysis patients, vascular calcification is associated with hypercalcemia, hyperphosphatemia and elevated calcium and phosphorus and ingested calcium.[4] Atherosclerosis of the ascending aorta is a leading cause of cerebrovascular accidents (CVA) in patients who undergo coronary artery bypass grafting (CABG). However, the ascending aorta is considered untouchable only in cases of severe calcification.[5] There are various techniques to deal with UAA like ascending aorta graft replacement, use of fibrillatory arrest, no touch technique and no pump technique but no touch and no pump techniques are considered least aggressive and dangerous and are widely used. In patients with porcelain aorta, manipulation of the thoracic aorta during cardiac surgery, such as incision, cross-clamping, or cannulation, leads to an increased risk of perioperative embolic stroke. Severe circumferential calcification of the thoracic aorta is called “porcelain aorta” and its presence can preclude safe aortic cross-clamping, arterial cannulation and other procedures during cardiac surgery. Porcelain aorta was defined as nearly or completely circumferential calcification of the ascending aorta and/or aortic arch.
Amorim et al. suggested the following classification of aortic calcification and how to approach porcelain aorta in cardiac surgery.[6] Type I is circumferential calcification in the ascending aorta. Type IA means there is no possibility of clamping the calcified aorta. Porcelain ascending aorta is characterised by calcifications of the entire circumference, making it impossible to perform ascending aortic clamping and other aortic treatments. Type IB means clamping may be possible at increased risk, and defined as the ratio of the circumferential length of calcification to the entire ascending aortic circumference below 75%. Type II is calcification of the descending aorta including or not the aortic arch, without the involvement of the ascending aorta. For the assessment of the ascending aorta, the preoperative chest radiograph and coronary angiograph are carefully evaluated in search of aortic calcifications. Moreover, intraoperative aortic palpation is routinely performed according to the method described by Mills and Everson, after systemic heparinisation, a 40- to 50-mm Hg drop in systemic pressure is induced and the aorta is gently palpated.[7]
In this case, we used ENCLOSE II device to perform proximal coronary anastomosis. The advantage of this method is that the Enclose®II anastomosis assist device facilitates the anastomosis of arterial side branches to the artificial graft (1) by eliminating the use of partial clamp on the artificial conduits and (2) by providing a plane surface for easy handling for suture.[3]
| Degree of ascending aorta disease | Definition |
|---|---|
| Absent | -- |
| Mild | Minor pathological conditions affecting the aorta, which could be prevented with proper placement of the aortic cannula and bypass grafts, are areas of concern. |
| Moderate | Diseases of significant extent raising concerns about potential embolisation, yet offering sufficient soft, disease-free regions for cannulation or placement of bypass grafts, are noteworthy |
| Severe | A notable circumferential disease requiring aortic cannulation, aortic cross-clamping and the insertion of bypass grafts into the affected ascending aorta is evident. |
Table 1. Mills and Everson criteria for grading ascending aorta atherosclerosis
Case report
A 56-year-old female presented with complaints of angina after minimal activity for 2 weeks, which was sudden in onset and progressively increased to angina at rest. She also had dyspnea, which was initially present on moderate physical activity but progressed gradually to dyspnea at rest more on lying supine. She was on treatment for hypertension for 10-12 years and was a CKD patient on dialysis for one year. After hospitalisation with these complaints, she was thoroughly investigated and coronary angiography revealed Triple vessel coronary artery disease with significant stenosis in LAD, OM and RCA. Chest X-ray revealed concentrically calcified ascending aorta and Carotid Doppler also revealed significant calcification in carotid arteries. CT head was also done which confirmed the calcification of most of the vessels.
After a thorough evaluation, she was planned to undergo Coronary Artery Bypass Grafting. On the day of surgery during the insertion of the arterial line, the radial artery was also found to be highly calcified, and thus the arterial line was inserted with the help of Doppler. The patient was shifted to the operation theatre and Off-Pump CABG surgery was performed using a midline sternotomy incision. The aorta was palpated and based on Mills and Everson Criteria; she had a moderate grade of ascending aortic calcification. Intraoperative TEE also confirmed the significant degree of calcification of the ascending aorta. The coronaries were then inspected and RCA was found to be nongraftable. The patient was initially planned for grafting using both LIMA and RIMA, but RIMA was not used since- (1) She had a severely osteoporotic bone; thus b/l mammary harvesting could have hampered the bone healing. (2)RCA was nongraftable and thus suitable RIMA-RCA anastomosis site could not be found
It has been said that the rate of these complications is higher if bilateral Internal Mammary Arteries (IMAs) have been harvested in a case of coronary artery bypass grafting, especially if harvested with a pedicle because it compromises the blood supply to the sternum. However, the risk of sternal dehiscence decreases if we use bilateral Robiscek repair with four to five interlocking figures of eight wires for sternal closure.[8] The patient had multiple reasons that would have hampered bone healing, thus, only LIMA harvesting was done
LIMA was then harvested and was anastomosed with LAD. A saphenous vein was harvested from the left leg and RSVG was anastomosed distally with OM. As the ascending aorta had moderate grade calcification with most of the area as hard and calcified as a rock, only a small soft part of the aorta could be found. Thus, it was decided to use ENCLOSE-II device for the proximal anastomosis. The ENCLOSE II device was fixed on the soft part of the aorta. (as seen in the figure) The upper and lower jaws of the device were opened and haemostasis was attained by clipping the artificial graft. Next, an anastomosis port to which the RSVG was to be anastomosed was created in the aorta using a 4.0mm puncher. The RSVG to OM graft was then anastomosed proximally to the aorta. RSVG to RCA grafting could not be done as the right coronary was nongraftable and also there was a discrepancy in vain size and LIMA size, thus, piggyback grafting could not be done.
The surgery went uneventful after which the patient was shifted to CTVS ICU. She was extubated on her post-operative day and showed no features of any embolisation in further post-operative days. Her post-op recovery was satisfactory, though she had a little extended stay as she developed pleural effusion due to fluid overload status because of CKD, but it was resolved after 2-3 sessions of dialysis and hence she was discharged hemodynamically and neurologically stable condition on her 9th postoperative day. She also came for follow-ups and had a normal recovery course.
Discussion
The total or subtotal atherosclerotic involvement of ascending aorta acts as a challenge in patient’s undergoing CABG due to increased risk of intraoperative and postoperative complications. According to various studies it has been seen the increased incidence of embolic stroke, sternal wound dehiscence or postoperative MI in patients undergoing CABG without proper planning for aortic clamping, proximal anastomosis or the off pump or on pump technique to be applied.
Due to the potential to radically modify the surgical strategy, the preoperative recognition of unclampable aorta and proper strategy planning becomes an important step. The advantage of using Enclose II anastomosis assist device is that it facilitates the anastomosis of conduit on aorta by eliminating the use of partial clamp on the artificial conduits and by providing a plane surface for easy handling for suture
Thus, in our case after evaluating the severity of aortic calcification and considering the increased risk of posteoperative stroke, the Enclose II anastomosis assist device was planned for use. Our patient had a moderate level of aortic calcification, so the use of Enclose II anastomosis device in the small soft part of aorta acted as a crucial technique for anastomosis of saphenous vein conduit, by providing a good operative field and eliminating application of partial aortic clamp, thus, reducing the risk of perioperative complications and helping in easier and faster proximal anastomosis.
LIMA was then harvested and was anastomosed with LAD. A saphenous vein was harvested from the left leg and RSVG was anastomosed distally with OM. As the ascending aorta had moderate grade calcification with most of the area as hard and calcified as a rock, only a small soft part of the aorta could be found. Thus, it was decided to use ENCLOSE-II device for the proximal anastomosis. The ENCLOSE II device was fixed on the soft part of the aorta. (as seen in the figure) The upper and lower jaws of the device were opened and haemostasis was attained by clipping the artificial graft. Next, an anastomosis port to which the RSVG was to be anastomosed was created in the aorta using a 4.0mm puncher. The RSVG to OM graft was then anastomosed proximally to the aorta. RSVG to RCA grafting could not be done as the right coronary was nongraftable and also there was a discrepancy in vain size and LIMA size, thus, piggyback grafting could not be done.
The surgery went uneventful after which the patient was shifted to CTVS ICU. She was extubated on her post-operative day and showed no features of any embolisation in further post-operative days. Her post-op recovery was satisfactory, though she had a little extended stay as she developed pleural effusion due to fluid overload status because of CKD, but it was resolved after 2-3 sessions of dialysis and hence she was discharged hemodynamically and neurologically stable condition on her 9th postoperative day. She also came for follow-ups and had a normal recovery course.
Compliance with ethical standards
Conflict of interest: The authors declare that they have no conflict of interest.
Consent: Informed consent was obtained
Ethical approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.

Figure 1: Preoperative Chest X-ray showing calcified aortic knuckle
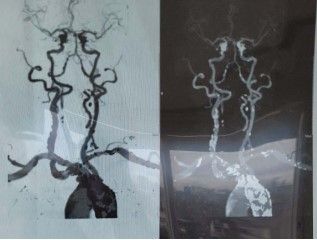
Figure 2: neck vessels showing calcification of carotid artery and other vessels

Figure 3(a): ENCLOSE II Device used for the surgery
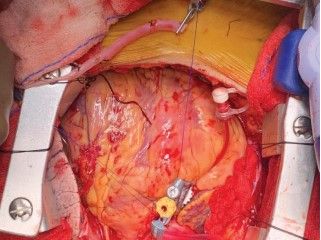
Figure 3(b): Intraoperative photograph during anastomosis showing application of ENCLOSE II device on soft part of ascending aorta

Figure 4(a): Intraoperative TEE Midesophageal ascending aortic view in short axis showing atheromatous aortic disease
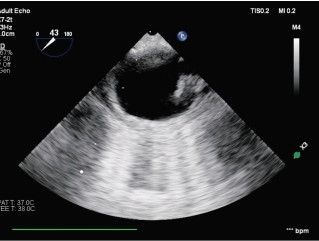
Figure 4(b): Intraoperative TEE Midesophageal Descending aortic view in short axis showing large atheroma
References
- Gaudino M, Glieca F, Alessandrini F, Luciani N, Cellini C, Pragliola C, Possati G. The unclampable ascending aorta in coronary artery bypass patients: A surgical challenge of increasing frequency. Circulation. 2000 Sep 26;102(13):1497- 502. doi: 10.1161/01.cir.102.13.1497. PMID: 11004139
- Osaka S, Tanaka M. Strategy for Porcelain Ascending Aorta in Cardiac Surgery. Ann Thorac Cardiovasc Surg. 2018;24(2):57-64. doi:10.5761/atcs.ra.17-00181
- Kikuchi K, Tambara K, Yamamoto T, Yamasaki M, Hirose H, Amano A. The Use of Enclose(®)II Anastomosis Assist Device for the Proximal Coronary Branch Anastomosis to Vascular Graft. Ann Vasc Dis. 2010;3(1):84-86. doi:10.3400/ avd.AVDhdi08023
- Mizobuchi M, Towler D, Slatopolsky E. Vascular calcification: the killer of patients with chronic kidney disease. J Am Soc Nephrol. 2009 Jul;20(7):1453-64. doi: 10.1681/ ASN.2008070692. Epub 2009 May 28. PMID: 19478096
- Gülcan O, Türköz R, Demirturk OS, Oguzkurt L, Türköz A. Extending the boundaries of no-touch aorta technique usage for coronary artery bypass grafting in patients with diseased ascending aorta. J Cardiovasc Surg (Torino). 2008 Jun;49(3):351-7. PMID: 18446121
- Amorim PA, Penov K, Lehmkuhl L, Haensig M, Mohr FW, Rastan AJ. Not all porcelain is the same: classification of circular aortic calcifications (porcelain aorta) according to the impact on therapeutic approach. Thorac Cardiovasc Surg. 2013 Oct;61(7):559-63. doi: 10.1055/s-0032-1333204. Epub 2013 Mar 8. PMID: 23475797
- Mills NL, Everson CT. Atherosclerosis of the ascending aorta and coronary artery bypass. Pathology, clinical correlates, and operative management. J Thorac Cardiovasc Surg. 1991 Oct;102(4):546-53. PMID: 1681138
- Singh S, Ralhan S, Sanyal A, Parage F, Sisodia V, Lohchab S. Prevention of Sternal Dehiscence Following Use of Bilateral Internal Mammary Arteries in OPCAB. World Journal of Cardiovascular Surgery 2020;10:254-263. doi: 10.4236/ wjcs.2020.1012027