

A 54-year-old female presented in OPD with very poor vision in both eyes. She had a history of recurrent redness with pain diagnosed as recurrent uveitis and high intraocular pressure in the past and was on topical steroids and antiglaucoma drops. She had high pathological myopia since childhood and wore thick glasses until she could see a year back. She had a family history of high myopia and glaucoma on her maternal side.
Clinical Findings:
Right eye: Visual Acuity: PL only/ PR accurate, Seclusio pupillae, Complicated Cataract, IOP 26 on 2 antiglaucoma drops, No retina view (Fig 1)
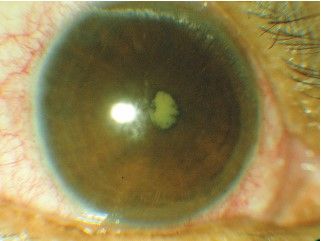
Figure 1 : Fig 1-Right eye -Preop-Visual Acuity -PL only, uveitic glaucoma, seclusio pupillae +complicated cataract in high myopic eye
Left Eye: Visual Acuity: 6/36 /Refractory Uveitic Glaucoma, Cup disc ratio of optic nerve head 0.8V:1, IOP 28 on 4 antiglaucoma drops
Pre-Operative planning
Cataract surgery in uveitic glaucoma and high myopia requires careful and meticulous planning.
IOP control was done before surgery to bring the intraocular pressure as low as possible by giving maximum antiglaucoma drugs and hyperosmotic agents before the cataract surgery
Oral and topical steroids were started a week prior to prevent inflammation postoperatively.
A complete workup done by a rheumatologist for uveitis was done. The patient was found to be HLA positive with ankylosing spondylitic changes and was put on oral immunosuppressants
Retina periphery checkup is a must in high myopia, but could not be done due to dense cataract and hence planned for the postoperative period once the media cleared up Optical Biometry to calculate IOL power was not possible due to seclusion pupillae and dense hypermature cataract so we took the biometry readings from A Scan and keratometry. These readings were then fed into Lenstar, and IOL power was calculated. The intraocular lens was in minus power and hence customized (Fig 2)
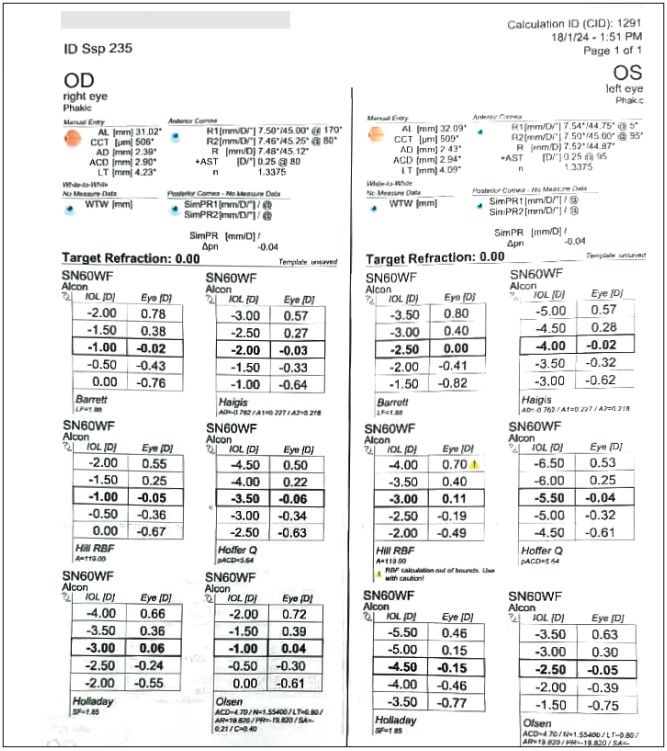
Figure 2 : Biometry to calculate IOL power
Stanby IOLs anterior vitrectomy are kept ready to deal with any change of plan or complication.
For the left eye, we planned Ahmed Glaucoma Valve surgery to control the intraocular pressure after two weeks.
Preoperative considerations - Right Eye:
Choice of anesthesia-Cataract surgery is usually made in topical anesthesia (drops), but in complicated cases, local peripbulbar anesthesia makes the surgery safer. We avoid giving large volumes of local anesthesia and massage as this may further jeopardize the optic neuropathy.
Posterior synechiae were released, and Iris Hooks were used to stretch open the pupil for visibility and phacoemulsification (Fig 3)
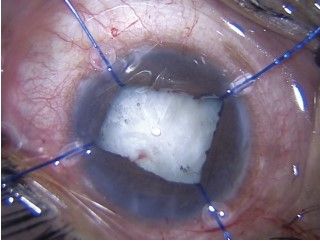
Figure 3 : Right eye -Perop-Flexible Iris Retractors used to stretch open the pupil to do phacoemulsification
Use high molecular weight dispersive viscoelastic to protect corneal endothelium.

Figure 4 : Right eye -Phacoemulsification to remove complicated cataract Iris hooks
Slow-mo low fluidics phacoemulsification are done to remove cataracts. (Fig 4)
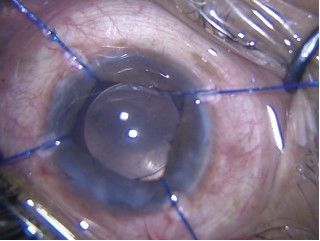
Figure 5 : Right eye –PerOp -Foldable Intraocular Lens inserted in capsular bag
Thorough cortical cleanup is necessary, followed by foldable intraocular lens implantation (Fig 5)
Postoperatively:
The patient did very well, with a Visual Acuity of 6/9 (Fig 6)
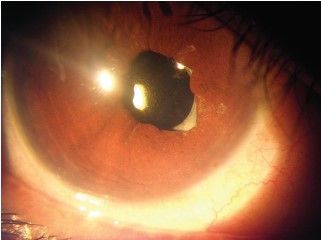
Figure 6 : Right eye -Postop-Visual Acuity 6_9, Pseudophakia, glaucoma controlled with eye drops
Postoperative considerations
Topical steroids should be cautiously used, and IOP monitoring must be done
It is advised to avoid the prostaglandin group of antiglaucoma drops as they may cause cystoid macular oedema post-cataract surgery, especially in a patient with a history of uveitis.
Through fundus examination was done to rule out any optic nerve and retinal pathology
Left eye:
Glaucoma valve surgery was planned after two weeks of operating the right eye
Pre Op Considerations:
Hyperosmotic agents were used to bring the IOP down before valve surgery. I V Mannitol 350ml was given an hour prior. This is done to avoid sudden hypotony-related complications during surgery.
Per Op Considerations:
AGV is primed before implanting. (Fig 7) in the pocket created superonasal under tenon between the recti muscles. A scleral flap is created to cover the tube partially, and the anterior edge is trimmed to insert in the anterior chamber. The valve is sutured onto the sclera.
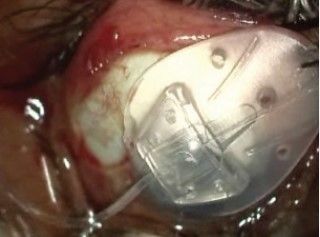
Figure 7 : Left eye -Ahmed Glaucoma Valve Surgery for Refractory Glaucoma
Post-Operative:
The Ahmed glaucoma valve was functional and able to control the intraocular pressure to 8mmhg after two weeks (Fig 8)
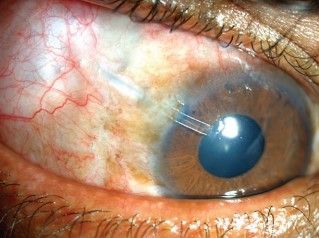
Figure 8 : Left eye -Tube of Ahmed Glaucoma valve well placed in the anterior chamber
Summary:
Meticulous planning is required when multiple eye diseases coexist. A careful preoperative assessment, perfect execution of surgery, and vigilant postoperative care ensure quality vision for patients. Counselling and discussing the prognosis need for long-term follow-ups is important to be discussed with the patient and their family.
Ruchi Rastogi1*, Subhash Gupta2, Dhaval Kumar Solanki1
, Bharat Aggarwal1