

Abstract: We report a case of 56-year-old male with known case of Hypertension and Hypothyroidism presented with complaints of generalised weakness and weight loss since 8 months (approx. 40kg), tightening in and around the mouth and hoarseness of voice with dysphagia since 6 months, swelling in feet since 3 months, cough and constipation on and off since one month. The laboratory results indicated that the serum calcium (S.Ca2+) level was 14.1 mg/dl and the ionized calcium (Ca2+) level was 1.62 mmol/l. Immunoglobulins were low {IgA- 17 mg/dl (50-410 mg/dl), IgG- 386 mg/dl (650-1500 mg/dl), IgM- 20 mg/dl (60-280 mg/dl); Immunofixation electrophoresis (IFE) revealed positive result for lambda free light chain (Figure 1) and further quantitative value lambda free light chain was high (Lambda free - 2054.89 mg/l). Whole Body FDG PET Scan revealed non-FDG avid lytic lesions at multiple bone sites. In view of suspicion of Multiple Myeloma, bone marrow aspiration and trephine biopsy were done which confirmed the diagnosis of Multiple Myeloma. ECG showed low voltage QRS complexes and 2D echo revealed- Global LVEF 55-60%, Dilated LA, concentric LVH with altered myocardial echotexture, no RWMA, Grade II diastolic dysfunction present (raised LVEDP), RVSP-39mmhg (moderate PAH), findings S/O- cardiac amyloid; which was later confirmed with Cardiac MRI. Abdominal fat pad biopsy revealed area of necrosis but negative for congo red stain (amyloidosis). The patient underwent VCD (bortezomib; cyclophosphamide; dexamethasone) chemotherapy with Daratumumab. By the time of publication, the patient had received autologous stem cell transplantation and after 10 courses of VCD with Daratumumab, repeat bone marrow aspiration and histo-biopsy revealed complete remission of myeloma. The uncommon Multiple Myeloma complication in this clinical case was associated with restricted cardiomyopathy as a result of secondary cardiac amyloidosis. This is true for both Multiple Myeloma and cardiac amyloidosis. When one of these diagnoses is initially established, more investigation should be done to rule out the other illness, keeping in mind the necessity of meeting standard diagnostic criteria and the challenge of conducting an effective diagnostic workup in occasionally complex clinical situations.
Introduction
The hallmark of multiple myeloma (MM) is usually the neoplastic growth of plasma cells that generate monoclonal immunoglobulin. The plasma cells multiply in the bone marrow, causing osteolytic lesions, osteopenia and/or pathologic fractures as well as significant skeletal damage. The cardiovascular system is one of the organs and systems that are implicated in the clinical picture of multiple myopathy. 10-15% of MM patients may experience severe side effects, such as localised or systemic AL amyloidosis, in addition to the underlying disease[2]. There are little worldwide statistics on cardiac amyloidosis and overt multiple myeloma (MM). Nicolaes Fonteyn first reported the disease known as amyloidosis in 1639. It is a collection of clinical disorders brought on by the deposition of soluble immunoglobulin light chains as insoluble fibrils[2,4]. Any organ, including the heart, neurological system, skin and subcutaneous tissue, kidneys and liver, can be impacted by systemic amyloidosis[2,3]. Proteinaceous components resulting from immunoglobulin light chain and transthyretin (TTR), also referred to as prealbumin, can deposit and cause cardiac amyloidosis[5]. Transport thyroid hormone and retinol combine to generate the TT. The National Centre for Health Statistics in the United States reports that there are 4.5 instances of AL amyloidosis for every 100,000 people[5].
The heart (70– 80%), kidneys (74%), liver (27%) and peripheral and autonomic nervous systems (22 and 18%, respectively) are the primary the target organs in AL amyloidosis[6,7] disease. Furthermore, isolated cardiac amyloidosis, an uncommon symptom, is only seen in 5% of individuals[8,9]. Clinical signs of AL cardiac amyloidosis include progressive chronic heart failure (HF) with ascites in the later stages, pleural effusion, peripheral edema in 70% of patients and severe rest dyspnea in 80% of patients[10]. Inhibiting abnormal precursor protein synthesis and plasmocyte proliferation is the main treatment strategy for cardiac amyloidosis in both MM and AL patients. The firstline therapies for MM and systemic AL amyloidosis consist of combining proteasome inhibitors (PIs; bortezomib, carfilzomib, and ixazomib) with other chemotherapeutic medications (cyclophosphamide, melphalan, and dexamethasone) as per guidelines for diagnosis and treatment[9,11]. Proteasome inhibition, however, can also occur in normal cardiomyocytes and/or endothelial cells, in addition to pathogenic plasma cells. This could lead to the development of cardiovascular toxicity. Clinical symptoms can include a decline in systolic function, ischemia development, including myocardial infarction (MI) and other rhythm/ conduction disorders[12,13]. The cardiotoxic effects of glucocorticoids and alkylating medications (cyclophosphamide and melphalan) are comparable[13]. Up to 4% of patients get HF while on bortezomib medication; however, if glucocorticoids are taken concurrently, this incidence can rise to 15%[13,14]. This clinical case report presents a patient diagnosed with multiple myeloma (MM), whose condition was further complicated by severe cardiac AL amyloidosis. It also highlights the intricacy of managing the patient’s treatment following the latest cardiooncology guidelines.
Case presentation
A 56-year-old male with known case of Hypertension and Hypothyroidism presented with complaints of generalized weakness and weight loss since eight months (approx. 40kg), tightening in and around the mouth and hoarseness of voice with dysphagia (only to solids, can tolerate liquid/soft diet) since six months, swelling in feet since three months, cough and constipation on and off since one month. Patient had a family H/O cardiovascular disease. Rest general and systemic examination was normal except for Bilateral pitting pedal edema and macroglossia (USG neck and MRI face and neck revealed: diffuse bulky intrinsic muscle of the tongue). The laboratory results revealed a haemoglobin (HB) level of 12.3 mg/dl, a total leukocyte count (TLC) of 7.6 (10^9/L), and a platelet count (PLT) of 273 (10^9/L), with normal liver and kidney function tests, including urinary calcium. However, the serum calcium (S.Ca2+) was elevated at 14.1 mg/dl, and the ionized calcium (Ca2+) level was 1.62 mmol/l. Immunoglobulin levels were found to be low, with IgA at 17 mg/dl (normal range: 50-410 mg/dl), IgG at 386 mg/dl (normal range: 650-1500 mg/dl), and IgM at 20 mg/dl (normal range: 60-280 mg/dl). Additionally, Beta-2 microglobulin was significantly elevated at 7.784 (normal range: 0.9-2.7). Immunofixation electrophoresis (IFE) revealed positive result for lambda free light chain {FIG 1} and further quantitative of value lambda free light chain was high (Lambda free - 2054.89 mg/l). Whole Body FDG PET Scan revealed multiple non-FDG avid lytic lesions involving bilateral scapulae, body of sternum, bilateral clavicles, bilateral acetabulum, D5, D6, L3 & L5 vertebral bodies, left 12th rib posteriorly, left ala sacrum, bilateral iliac bones and bilateral proximal femur. In view of suspicion of Multiple Myeloma, bone marrow aspiration and trephine biopsy were done which revealed 70% plasma cells and 90% CD138 positive plasma cells of all nucleated cells {hypercellularity (90%)} respectively, features consistent with plasma cell myeloma.
Meanwhile, baseline ECG was obtained which showed low voltage QRS complexes, ectopics with ST depression in anterolateral leads and T-wave inversion in V3-V6(FIG.3); along with raised cardiac enzymes and 2D echo was done which revealed Global LVEF 55-60%, Dilated LA, concentric LVH with altered myocardial echotexture, no RWMA, Grade II diastolic dysfunction present (raised LVEDP), RVSP-39mmhg (moderate PAH), findings S/O- cardiac amyloid; which was later confirmed with Cardiac MRI (Figure 2).
| Laboratory results | 11/01/2023 | 21/01/2023 | 06/05/2023 |
|---|---|---|---|
| S. calcium (mg/dl) | 14.1 | 8.3 | 8.5 |
| Total Protein (g/dl) | 5.6 | 5.4 | 4.4 |
| Creatinine (mg/dl) | 1.0 | 0.8 | 0.6 |
| Ionised Calcium (mmol/l) | 1.62 | 1.35 | |
| Trop-I (ng/ml) | 0.17 | 0.15 | |
| NTproBNP (pg/ml) | 6432 | 4737 | 2370 |
| eGFR (ml/min/1.73 m²) | 77.19 | 99.85 | 139.02 |
Table 1: Laboratory results of the case presentation
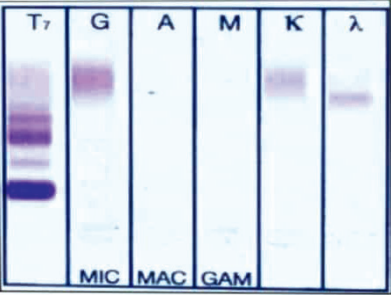
Figure 1: Immunofixation electrophoresis (IFE) revealed positive result for lambda free light chain corresponding to suspicious M spike
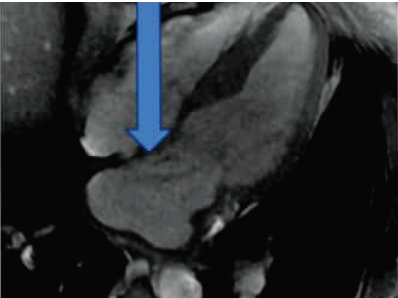
Figure 2(A): Myocardial enhancement suggestive of infiltration and likely amyloidosis
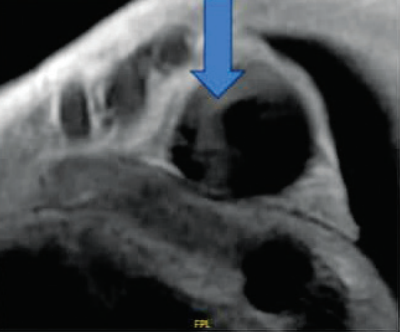
Figure 2(B): Dilated left atrium
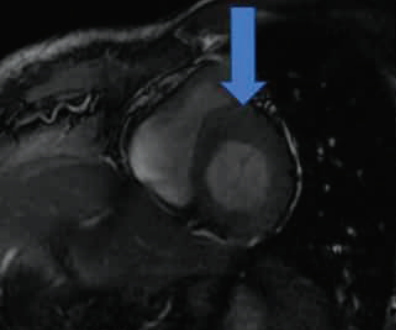
Figure 2(C): Concentric hypertrophy of left ventricle
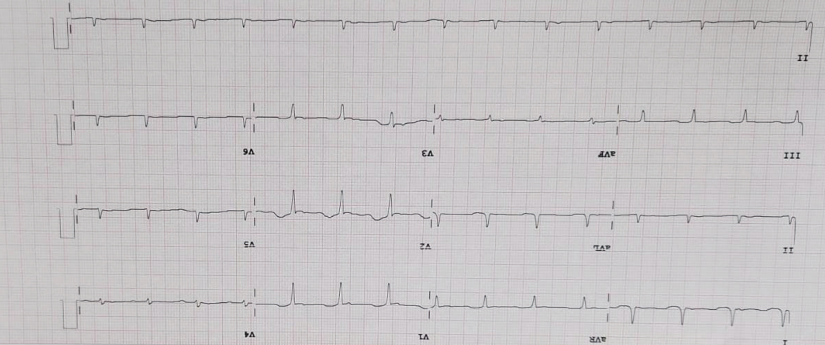
Figure 3: 12 lead ECG showed low voltage complexes, ectopics with ST depression in antero-lateral leads and T-wave inversion in V3-V6
US guided trucut biopsy of abdominal fat pad was done which showed mature fat with areas of fat necrosis. No apple birefringence under polarised light with Congo Red staining (negative for amyloid), but the combination of clinical features (macroglossia, bilateral pedal edema, hoarseness of voice, fatigueness) along with cardiovascular findings (including ECG, 2d-Echo and Cardiac MRI) in the background of Multiple Myeloma was highly suggestive of Cardiac Amyloidosis. The pathological biopsy is the only means to confirm myocardial amyloidosis, but negative results of Congo-red staining do not rule out myocardial amyloidosis[15]. So patient was diagnosed as a case of Multiple Myeloma with Cardiac Amyloidosis.
Treatment
The Patient was started on specific treatment, Inj. Dexamethasone 20mg. Diuretics are the mainstay of supportive care in cardiac amyloidosis. Torsemide [20mg, twice daily] and Spironolactone (50mg, twice daily) were used to alleviate cardiac pre-load and edema. Autologous stem cell transplantation was done after 3 months. After 6 months and 10 courses of Daratumumab with Bortezomib, cyclophosphamide and dexamethasone (VCd), repeat bone marrow aspiration and histo-bone marrow biopsy showed - plasma cells accounted for 3% of the cell count on flow cytometry & CD138 positive plasma cells are 1% of all nucleated cells, respectively; with the patient showing complete remission.
Discussion
Multiple Myeloma and Amyloidosis are two distinct but related entities that use distinct pathogenetic processes to inflict damage and failure in important target organs[15]. Globally, there is variation in their estimated occurrence. In general, the incidence of MM is roughly five times higher than that of AL. For example, in Spain, the estimated crude incidence of Amyloidosis in 2018 was 1.19/100,000 person-years 18, while incidence rate of MM in the last ten years was approximately 5/100,000 person- years. The estimated crude incidence in 2021 was 6.7[16,17]. Insoluble homomeric amyloid fibrils, which are made up of different serum proteins, progressively replace normal tissue in different human organs as a result of the systemic, organ-limited disease amyloidosis[19]. Six subtypes of major heart related amyloidosis can be distinguished in the clinical setting, (1) AL, or primary amyloidosis; (2) AA or secondary amyloidosis; (3) familial (hereditary) am yloidosis; (4) senile systemic amyloidosis, also referred to as wild type transthyretin; (5) isolated atrial amyloidosis; and (6) haemodialysis-related amyloidosis, which is caused by beta-2 microglobulin accumulation20. Out of all patients exhibiting cardiac dysfunction, fewer than 5% have familial syndrome s, 10% have AA amyloidosis and up to 50% have AL amyloidosis21. Patients with AL amyloidosis is diagnosed at an average age of 64 years old[24].
The pericardium, endocardium and conduction system may also be affected by amyloid depositions, which primarily affect the interstitium of the contractile myocardium[25]. A poor prognosis is generally associated with significant morbidity when there is cardiac involvement[26,28]. Early diagnosis and vigorous treatment of plasma cell dyscrasia may change prognosis in cases of cardiac amyloidosis (CA), i.e. with chemotherapy and autologous stem cell transplantation improve clinical outcomes[29,30].
Our patient was a tall, 56-year-old male who arrived complaining of pedal edema, dysphagia and voice hoarseness along with loss in weight. It is crucial to stress that even while systemic lightchain amyloid illness only affects 10% of individuals with multiple myeloma, their prognosis is very bad, particularly if they also have cardiac amyloidosis[22,23]. Patient was evaluated and serum calcium was found to be 14.10, lambda free chain in serum was found to be very high, serum electrophoresis showed no M spike and PET CT showed Non FDG avid osteolytic lesion of bone at multiple sites. Following evaluation, a bone marrow sample was performed, confirming the multiple myeloma diagnosis.
ECG, echocardiography and cardiac MRI are also important proofs for the diagnosis of myocardial amyloidosis. A study describing the clinical characteristics of eight patients with cardiac amyloidosis caused by MM found that seven cases out of eight (87.5%) showed low li mb lead voltage, six (75.0%) cases had poor precordial R-wave progression or pseudonecrotic Q wave and three (37.5%) cases present with ST-T wave abnormalities[32]. Studies have shown that the most characteristic ECG manifestation in patients with myocardial amyloidosis is the low-voltage pattern[31]. Typical echocardiography is characterised by thickening of the left ventricular wall with a granular sparkling appearance in the absence of hypertension and a limited or diffuse tissue enhancement of the heart by gadolinium on MRI.
Congo Red staining of biopsy tissue can be used to confirm myocardial amyloidosis if results on echocardiography, MRI and ECG are positive. However, negative results from Congo Red staining do not rule out myocardial amyloidosis[15]. Although, blind examination of kidney, abdominal adipose and intestinal tissue are frequently employed in place of myocardial biopsy due to the poor heart function in patients with myocardial amyloidosis. The positivity rates of different tissue specimens stained with Congo Red were reported as follows, abdominal fat, 50–80%; bone marrow, 56%; rectum, 75%; kidney, 94%; carpal ligament, 82%; liver, 97%; small intestine, 83%; skin, 90%; sural nerve, 86% and heart, 100%. However, the buccal mucosa was the most common site of amyloid deposition in the oral cavity, followed by the tongue, palate, gingiva and floor of the mouth.
In this patient Abdominal Fat pad biopsy was done which revealed area of fat necrosis which was negative for Congo red stain and so for amyloid. The patient had indentations on the tongue and suffered from macroglossia. Taking patient’s wish into consideration, an invasive biopsy could not be taken.
But keeping the clinical features and imaging in mind, a diagnosis of multiple myeloma with cardiac amyloidosis was made and the patient was started on diuretics, chemotherapy and autologous stem cell transplantation. The Patient responded well to the treatment and repeat bone marrow histo-biopsy and aspiration revealed complete remission of myeloma and a normal MUGA scan post-chemotherapy. Hence proving that early diagnosis and treatment has a great impact on prognosis.
References
- Arnt V Kristen. Amyloid Cardiomyopathy. Herz (Cardiovascular Diseases). 2020 May;45(3):267-271
- Mirela Andrei, Jen Chin Wang. Cutaneous light chain amyloidosis with multiple myeloma: A concise review. Hematology/Oncology and Stem Cell Therapy. 2019 Jun;12(2):71-81
- Bouke P C Hazenberg. Amyloidosis: a clinical overview. Rheumatic Diseases Clinics of North America. 2013 May;39(2):323-45
- Rodney H Falk, Kevin M Alexander, et al. AL (Light-Chain) Cardiac Amyloidosis: A Review of Diagnosis and Therapy. Journal of the American College of Cardiology. 2016 Sep 20;68(12):1323-41
- Lauren G Gilstrap, Francesca Dominici, et al. Epidemiology of Cardiac Amyloidosis-Associated Heart Failure Hospitalizations Among Fee-for-Service Medicare Beneficiaries in the United States. Circulation: Heart Failure (AHA Journals) 2019 Jun;12(6):e005407
- Pablo Garcia-Pavia, Claudio Rapezzi, Yehuda Adler, et al. Diagnosis and treatment of cardiac amyloidosis: a position statement of the ESC Working Group on Myocardial and Pericardial Diseases. European Heart Journal. 2021 Apr 21;42(16):1554-1568
- Lucie Karafiatova, Tomas Pika. Amyloid Cardiomyopathy. Biomedical Papers of the Medical Faculty of the University Palacky, Olomouc, Czechoslovakia. 2017 Jun;161(2):117-127
- Giovanni Palladini, Paolo Milani, Giampaolo Merlini. Management of AL amyloidosis in 2020. Blood (American Society of Hematology-ASH) 2020 Dec3;136(23):2620-2627
- Michelle M Kittleson, Mathew S Maurer, et al. Cardiac Amyloidosis: Evolving Diagnosis and Management: A scientific statement from the American Heart Association. Circulation (AHA Journals). 2020 Jul 7;142(1):e7-e22
- Morie A Gertz. Immunoglobulin light chain amyloidosis: 2020 update on diagnosis, prognosis, and treatment. American Journal of Hematology. 2020 Jul;95(7):848-860
- M A Dimopoulos, P Moreau, E Terpos, et al. Corrigendum to Multiple Myeloma: EHA-ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of Oncology: official journal of the European Society for Medical Oncology. 2021 Mar;32(3):309-322
- Markus B. Heckmann, Shirin Doroudgar, et al. Cardiovascular adverse events in multiple myeloma patients. Journal of Thoracic Disease. 2018 Dec;10(Suppl 35):S4296-S4305
- Jose Luis Zamorano, Patrizio Lancellotti, et al. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). European Heart Journal. 2016 Sep 21;37(36):2768-2801
- Alessandra Cuomo, Alessio Rodolico, et al. Heart Failure and Cancer: Mechanisms of Old and New Cardiotoxic Drugs in Cancer Patients. Cardiac Failure Review-Radcliffe Cardiology. 2019 May;5(2):112-118
- Julian D Gillmore, et al. Guidelines on the diagnosis and investigation of AL amyloidosis. British Journal of Haematology. 2015 Jan;168(2):207-18
- D-Y-L Chang-Chan, R Rios-Tamayo, et al. Trends of incidence, mortality, and survival of multiple myeloma in Spain. A twenty-three-year population-based study. Clinical & Translational Oncology. 2021 Jul;23(7):1429-1439
- Estimaciones de la incidencia del cancer en Espana, 2021. Red Espanola de Registros de Cancer (REDECAN), 2021
- Nishant Kumar, Nicole J Zhang, et al. Global epidemiology of amyloid light-chain amyloidosis. Orphanet Journal of Rare Disease. 2022 Jul19;17(1):278
- Giampaolo Merlini, Vittorio Bellotti. Molecular mechanisms of amyloidosis. New England Journal Of Medicine. 2003 Aug 7;349(6):583-96
- Per Westermark, Merrill D Benson, et al. Amyloid: toward terminology clarification. Report from the Nomenclature Committee of the International Society of Amyloidosis. Amyloid - The International Journal of Experimental and Clinical Investigation: the official journal of the International Society of Amyloidosis. 2005 Mar;12(1):1-4
- Robert A. Kyle. Amyloidosis. Circulation (AHA Journals). 1995 Feb;91(4):1269-1271
- David Sedaghat, Ramzan M Zakir, et al. Cardiac Amyloidosis in a patient with multiple myeloma: a case report and review of literature. Journal of Clinical Ultrasound. 2009 Mar-Apr;37(3):179-84
- Angela Dispenzieri, Robert A Kyle, et al. Survival in patients with primary systemic amyloidosis and raised serum cardiac troponins. Lancet (London, England). 2003 May 24;361(9371):1787-9
- R A Kyle, M A Gertz. Primary systemic amyloidosis: clinical and laboratory features in 474 cases. Seminars in Haematology. 1995 Jan;32(1):45-59
- V Mathew, L J Olson, et al. Symptomatic conduction system disease in cardiac amyloidosis. American Journal of Cardiology. 1997 Dec 1;80(11):1491-2
- Morie A Gertz, Ray Comenzo, et al. Definition of organ involvement and treatment response in immunoglobulin light chain amyloidosis (AL): a consensus opinion from the 10th International Symposium on Amyloid and Amyloidosis, Tours, France, 18-22 April 2004. American Journal of Hematology. 2005 Aug;79(4):319-28
- S Vincent Rajkumar, Angela Dispenzieri, et al. Monoclonal gammopathy of undetermined significance, Waldenstrom macroglobulinemia, AL amyloidosis, and related plasma cell disorders: diagnosis and treatment. Mayo Clinic Proceedings. 2006 May;81(5):693-703
- Rodney H Falk. Diagnosis and management of the cardiac amyloidosis. Circulation (AHA Journals). 2005 Sep 27;112(13):2047-60
- M Grogan, M A Gertz, R A Kyle, et al. Five or more years of survival in patients with primary systemic amyloidosis and biopsy-proven cardiac involvement. The American Journal of Cardiology. 2000 Mar 1;85(5):664-5,A11
- Shameem Mahmood, Giovanni Palladini, et al. Update on treatment of light chain amyloidosis. Haematologica. 2014 Feb;99(2):209-21
- Keyur B Shah, Yoshio Inoue, et al. Amyloidosis and the heart: a comprehensive review. Archives of Internal Medicine. 2006 Sep;25166(17):1805-13
- Qisi Zhang, Yingli Qiao, et al. Myocardial amyloidosis following multiple myeloma in a 38-year-old female patient: A case report. Open Medicine (Wars). 2020;15(1):396-402