

Abstract: Filarial lymphedema (FLE) is the most common cause of secondary lymphedema, with endemic prevalence in developing countries. This has been traditionally managed conservatively with complex decongestive therapy (CDT) in early-stage and excisional surgery at late-stage. Results of Lympho-Venous Anastomosis (LVA) and post-oncological lymphedema have been encouraging, and it is currently a widely accepted surgical treatment. In this case report we demonstrate the planning and surgical steps along with the outcome of LVA in early-stage lower limb FLE. 32-year-old female with early-stage left lower limb FLE underwent two end-to-end lympho-venous anastomosis. Handheld ICG imaging was used to diagnose earlystage lymphedema and locate patent lymphatic channels for performing LVA.
Patient showed decreased limb volume from 22% to 4% with the combined approach of Complex Decongestive Therapy (CDT) and LVA. At the 3-month follow-up, patient gave an excellent outcome on subjective scoring with a significant reduction in man hours spent in bandaging. Our early experience showed that LVA may represent an effective treatment option in the multi-modality approach to early-stage lower limb FLE.
Introduction
Filariasis is the most common cause of lymphedema in the world with 120 million cases[1]. The disease is due to the parasite Wuchereria bancrofti acquired due to mosquito bites. The acute phase of the infection can be cured with oral albendazole or Diethyl Carbamazepine. However, delayed sequelae of the disease appear in the form of chronic lymphatic obstruction presenting as lymphedema.
These patients initially present with heaviness and tightness of the limb followed by pitting edema progressing from the ankle upwards. The edema is initially reducible with limb elevation, however progresses to non-reducible and non-pitting edema. Repeated cellulitis is a classical feature resulting in multiple hospital admissions. There is progressive deposition of adipose tissue and fibrosis which eventually leads to skin changes and disfigurement of the limb. Elephantiasis is the terminal stage which signifies a long standing untreated lymphatic obstruction.
Although most common cause is filariasis, there is an increasing incidence of post oncological nodal resection resulting in lymphatic obstruction. Incidence is as high as 21 % post mastectomy and 40% post uro-gynecological cancers[2,3]. There is an increasing awareness and need to address this issue as the incidence of cancer seems to be on the rise.
Treatment so far has been physiotherapy, which includes compression bandaging, manual lymphatic drainage, aerobic exercises, skin care and limb elevation. Cumulatively, these are referred to as complex decongestant therapy (CDT). The role of CDT in the management of lymphedema cannot be overemphasised. It is still the gold standard treatment protocol and a vital element of any successful lymphedema unit[4].
CDT primarily focuses on the optimal usage of the remaining lymphatic drainage of the limb. Thus, pushing further, the limits of an already over-burdened and exhausted lymphatic tracks. There is no new drainage pathway created and the patient is completely dependent on CDT. The hassle is the time and effort that goes daily to perform bandaging, cost of the specialised short stretch bandages and patient compliance. Although the results are reproducible and evident that the patient is dependent on bandaging for the rest of his or her life. Hence, arises the need to establish newer drainage pathways.
Plastic surgery and microsurgical procedures help create newer permanent alternate pathways for lymph drainage avoiding need for lifelong dependence on bandaging and CDT. There has been a fast-paced research and development of newer techniques for establishing lymphatic drainage. One of the procedures is Lymph venous anastomosis (LVA) described in the following case.
Case: Our patient is a 32-year female with left lower limb edema restricted below knee. Her symptoms involve heaviness and tightness of the limb. In the last year, she has presented with cellulitis twice, for which intravenous antibiotics were administered. Clinically, there is non-pitting edema over the dorsum of the foot without skin changes. Edema below the knee is partially reducible without any skin changes. Taiwan Lymphoscintigraphy staging showed partial obstruction with minimal ascent of the TC99 dye and delayed uptake in the inguinal nodes along with dermal backflow. Volume difference in the two limbs was 22 % (calculated using circumferential measurements and truncated cone formulae).
After a thorough examination and limb volume assessment, we started the patient on supervised CDT. After 2 weeks of CDT reduction her limb volume difference was down to 8%. The patient continued to experience subjective symptoms of limb heaviness and tightness. On average, she spends 8 hours a day bandaging and avoids outdoor activities during this period. Her primary concern was a reduction in the need for bandaging and preventing further progress of the disease. After counselling and discussing all the options available, she was planned for a Lymphovenous Anastomosis.

Figure 1: Pre-operative / Post-CDT Image – Left lower-Limb lymphedema. Volume difference of 8% between the two limbs up to the knee joint. Irreducible edema over the foot without skin changes
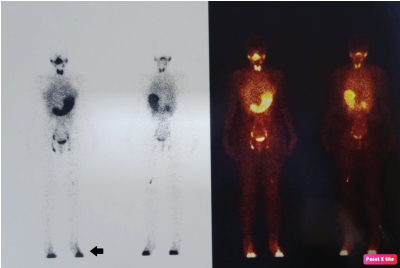
Figure 2: Lymphoscintigraphy - Showing minimal dermal backflow with delayed ascent to the inguinal lymph nodes
Introduction
Step 1: ICG imaging
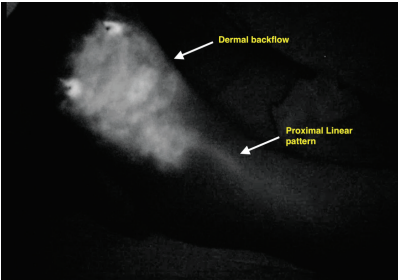
Figure 3: ICG image showing diffuse pattern of dermal backflow in the dorsum of the foot with moderate linear track in the leg proximal to the ankle joint
Step 2
The linear track was marked on the skin superimposed on the ICG images. Perpendicular incisions were planned over these linear tracks. Once we decided to go ahead with the procedure patient was induced under general anaesthesia and parts prepared. Iso-sulphane blue dye was injected 3 cm proximal to the planned incision site. The purpose of the dye was to highlight the lymphatic vessel under the microscope. Adrenaline infiltration was given at the incision site
Step 3
The incision is taken under optical magnification and dissection is done in the sub-dermal layer to locate a lymphatic vessel. After identifying the vessel, a venule is identified with a functional valve. The valve is essential to avoid and backflow of blood. Under magnification and using 11-0 ethilon sutures Lymphovenous anastomosis is performed. LVA was performed at 2 locations.

Figure 4: End to End Lympho-venous anastomosis
Immediate crepe bandage is applied on table. Patient started mobilising from the next day. Discharged on post-op day one. Gentle crepe bandages are continued for two weeks with skin care. Suture removal is done after two weeks.
Results
At four weeks post-operatively, the improvement is largely a subjective improvement. She feels that her leg is much lighter and softer. This is evident from the very next day. She feels her walking has improved and more convenient with resolution of dull aching pain. She started walking immediately and back to her job by just wearing a gentle crepe bandage. Need for her bandaging has reduced drastically, although we advise her to continue for few more weeks.
Follow up of 3 months
A subjective scoring was taken from patient based on the following 6 parameters.
- Limb Size
- Limb tightness
- Limb heaviness
- Need for bandaging
- Affect in activities of daily living
- Cosmetic appearance of the leg
Visual analogue scale was used to quantify the improvement.
| Parameters | Visual analogue scale (1 to 10) |
|---|---|
| 1. Reduction in limb size | 8 |
| 2. Reduction limb tightness | 9 |
| 3. Reduction limb heaviness | 9 |
| 4. Need for bandaging | 9 |
| 5. Affect in activities of daily livinge | 8 |
| 6. Cosmetic appearance of the leg | 8 |
Table 1: Percentage difference in limb volume was reduced to 4 %. Repeat lymphoscintigraphy and ICG image is planned at six months.
Discussion
Filarial lymphedema is a chronic and debilitating condition which results in progressive limb swelling/enlargement, heaviness and tightness. The limb is prone to repeated episodes of cellulitis and disease progression with skin changes. It has a profound impact on the quality of life and activities of daily living. The psychological impact on body image can be a social stigma affecting an individual’s self-confidence. With each episode of cellulitis, the disease progresses and eventually leads to limb deformity with an ulcer. Chronic fibrosis results in skin changes and irreversible injury of the lymphatic ducts.
The treatment so far has primarily been bandaging and is still the gold standard[4]. Supervised decongestive therapy is the cornerstone of the success of any lymphedema program. It optimises the existing lymphatic system and acts as an excellent tool for patient selection. The author would recommend to assess patient compliance to CDT prior to any form of surgical procedure as the best outcome is dependent on a continued supervised CDT post procedure.
When it comes to physiological surgeries in lymphedema, the primary objective is to establish an alternate drainage pathway for the lymph. Two procedures have been popularised in the recent decade and proven to be largely effective. Vascularised lymph node transfer (VLNT) involves placement of lymph node basins along with their vascular supply into the affected limb. The commonly used donor options are Supraclavicular VLNT, Sub-mental VLNT, Gastro-epiploic VLNT and Groin VLNT. Each of them has their advantages and drawbacks and becomes a matter of surgeon preference. However, the mechanism of action involves growth of newer afferent channels due to the release of VEGF 3 and the wick or sump like effect which helps them to absorb the free interstitial fluid[5.6.7]. The procedure requires 2-3 weeks of recovery period and latent phase for the growth of newer afferent channels. The results become more evident as the time passes. The advantage of this procedure is that it can be offered to individuals at all stages of lymphedema with varying outcomes depending upon the extent of fibrosis. Even in severe cases, there is reduction in the manhours spent in bandaging and preventing further progress of the disease[8].
Lympho-venous anastomosis is categorised as a supermicrosurgical procedure where a sub-dermal lymphatic is anastomosed to a sub-dermal venule. This provides an immediate drainage pathway for a congested and dilated lymphatic system[9]. The results are evident in the immediate post-op period with significant subjective improvement in limb heaviness and tightness. The procedure is performed through minimal incisions and patient can be mobilised from the very next day. Long term patency of the LVA which have also been demonstrated through imaging. LVA is a far less invasive surgery with immediate long-standing results compared to VLNT[10].
However, there are three hurdles when it comes to performing LVAs.
- Patient selection: Patients with reducible lymphedema without skin changes are ideal for the procedure (Stage 1 and 2), before major fibrosis sets in. As the pathophysiology suggest, in early-stage lymphedema due to back pressure the lymphatic ducts get dilated and hypertrophied. Hence, amenable to microvascular anastomosis. As the disease progresses with repeated attacks of cellulitis, the lymphatic channels become sclerotic. ICG imaging helps to show early patterns of dermal backflow which may be missed in lymphoscintigraphy
- Identification of the lymphatic channels: Handheld ICG cameras are essential and accurate for surface marking of lymphatic ducts. It is essential in planning the incision and increases chances of finding a lymphatic vessel. Isosuphane blue injected proximal to the incision site helps in identification of the lymphatic ducts under the microscope by giving it a light blue tinge.
- Super-microsurgery skill: The average size of these vessels is less than 0.7 mm. Magnification with help of a microscope is a must to conclusively identify a lymphatic vessel. Supermicro instrumentation and 10-0 or 11-0 ethilon suture are among the other essentials. And certainly, there is a steep learning curve, but a trained microsurgeon would find it achievable.
Through this case the author would like to highlight few key points
- Early diagnosis: Outcome of establishing a new physiological drainage becomes difficult and would require adding a reduction procedure like Charles excision with skin grafting, wedge excision or liposuction. In early stages minimally invasive procedures like LVA can be performed which provides excellent long-term results along with relief from CDT. ICG imaging helps to diagnose these patients early on and should be the investigation of choice.
- Role of CDT: It is the most important cog in the wheel. Preoperative optimisation and post-operative follow through is essential for any successful lymphedema surgery program.
- Microsurgical ecosystem: For a successful program an ecosystem which helps to deliver sustainable, reproducible and predictable results is essential. Super-microsurgery requires instrumentations and trained man power. High optical magnification, instrumentations, suture material and dyes are few of the essentials. Over a period training the staff and creating awareness for a stable referral system will help boost early diagnosis and treatment of lymphedema.
CONCLUSION:
Microvascular surgery completes the puzzle of lymphedema care. It does not replace the traditional physiotherapy but helps to provide an end point for lifelong compliance to bandaging. Lymphovenous anastomosis is a simple and a minimally invasive procedure for establishing a newer drainage pathway. Early diagnosis and patient selection, complementing with supervised CDT and realistic expectations can be corner stone to an effective lymphedema programme.
Supplemental material
Video 1- Detail review of patient planning and surgical procedure.
References
- Shenoy RK. Clinical and pathological aspects of filarial lymphedema and its management. Korean J Parasitol. 2008;46(3):119-125
- DiSipio T, Rye S, Newman B, Hayes S. Incidence of unilateral arm lymphoedema after breast cancer: a systematic review and meta-analysis. Lancet Oncol. 2013 May;14(6):500-15
- Hayes SC, Janda M, Ward LC, Reul-Hirche H, Steele ML, Carter J, Quinn M, Cornish B, Obermair A. Lymphedema following gynecological cancer: Results from a prospective, longitudinal cohort study on prevalence, incidence and risk factors. Gynecol Oncol. 2017 Sep;146(3):623-629
- Michopoulos E, Papathanasiou G, Vasilopoulos G, Polikandrioti M, Dimakakos E. Effectiveness and Safety of Complete Decongestive Therapy of Phase I: A Lymphedema Treatment Study in the Greek Population. Cureus. 2020 Jul 19;12(7):e9264
- Liu HL, Pang SY, Lee CC, et al. Orthotopic transfer of vascularized groin lymph node flap in the treatment of breast cancer-related lymphedema: Clinical results, lymphoscintigraphy findings, and proposed mechanism. J Plast Reconstr Aesthet Surg 2018;71:1033-40. 10.1016/j. bjps.2018.02.015
- Suami H, Scaglioni MF, Dixon KA, et al. Interaction between vascularized lymph node transfer and recipient lymphatics after lymph node dissection-a pilot study in a canine model. J Surg Res 2016;204:418-27. 10.1016/j.jss.2016.05.029
- Pappalardo M, Patel K, Cheng MH. Vascularized lymph node transfer for treatment of extremity lymphedema: An overview of current controversies regarding donor sites, recipient sites and outcomes. J Surg Oncol. 2018;117(7):1420–1431
- De Brucker B, Zeltzer A, Seidenstuecker K, Hendrickx B, Adriaenssens N, Hamdi M. Breast Cancer-Related Lymphedema: Quality of Life after Lymph Node Transfer. Plast Reconstr Surg. 2016;137(6):1673–1680
- Kareh AM, Xu KY. Surgical Management of Lymphedema. Mo Med. 2020 Mar-Apr;117(2):143-148
- Chang DW, Suami H, Skoracki R. A prospective analysis of 100 consecutive lymphovenous bypass cases for treatment of extremity lymphedema. Plast Reconstr Surg. 2013;132(5):1305–1314